I’m sorry, but there was an error in the previous post and I had to remove it. Depending on information received, I may be able to repost it.
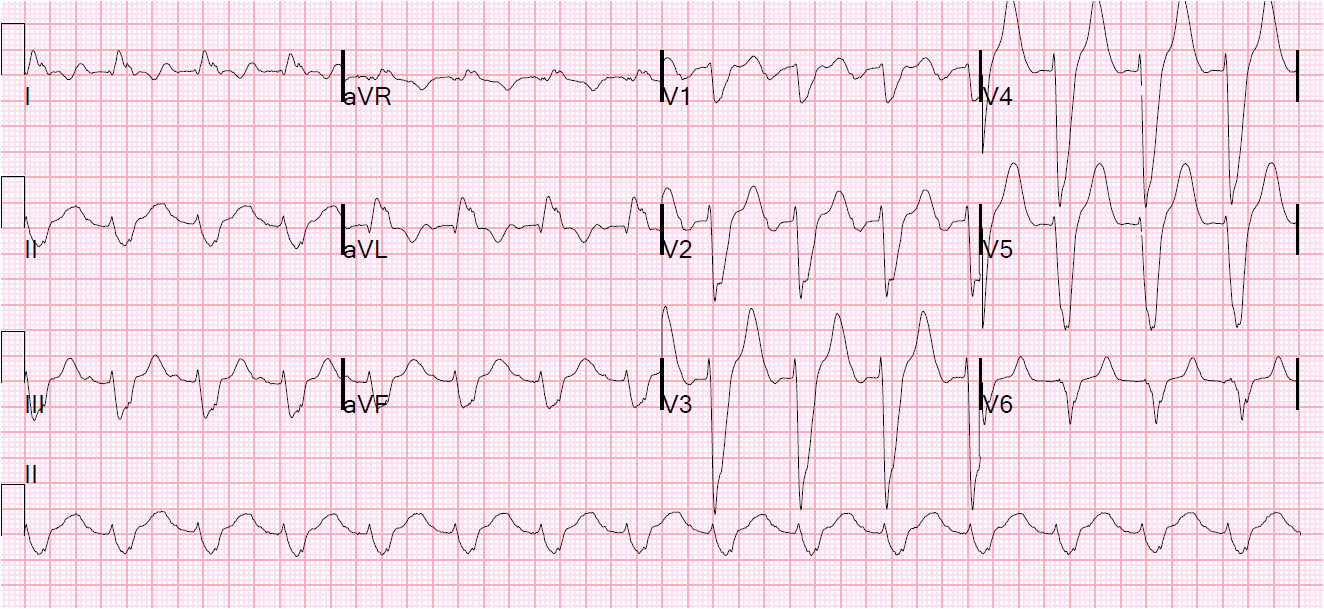
A dialysis patient presented with vomiting. He has known baseline left bundle branch block. Here is his initial ECG:
 |
|
|
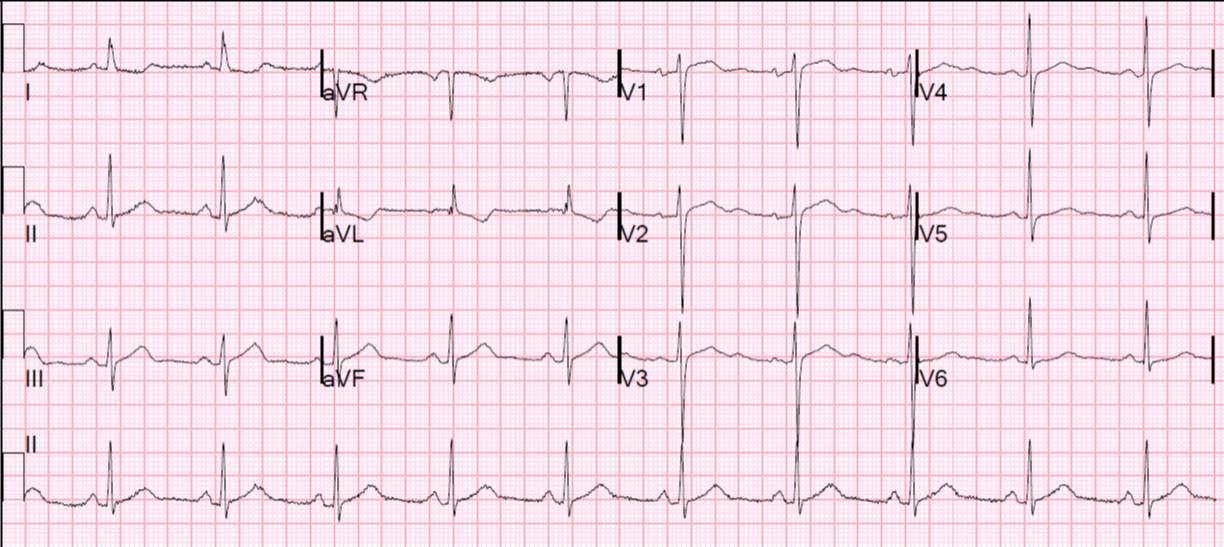
Here is his previous ECG, recorded with normal postassium:
 |
|
|
A widened QRS should always make you suspicious of hyperkalemia. Indeed, the potassium was 7.3 mEq/L. After therapy, the widening resolved.
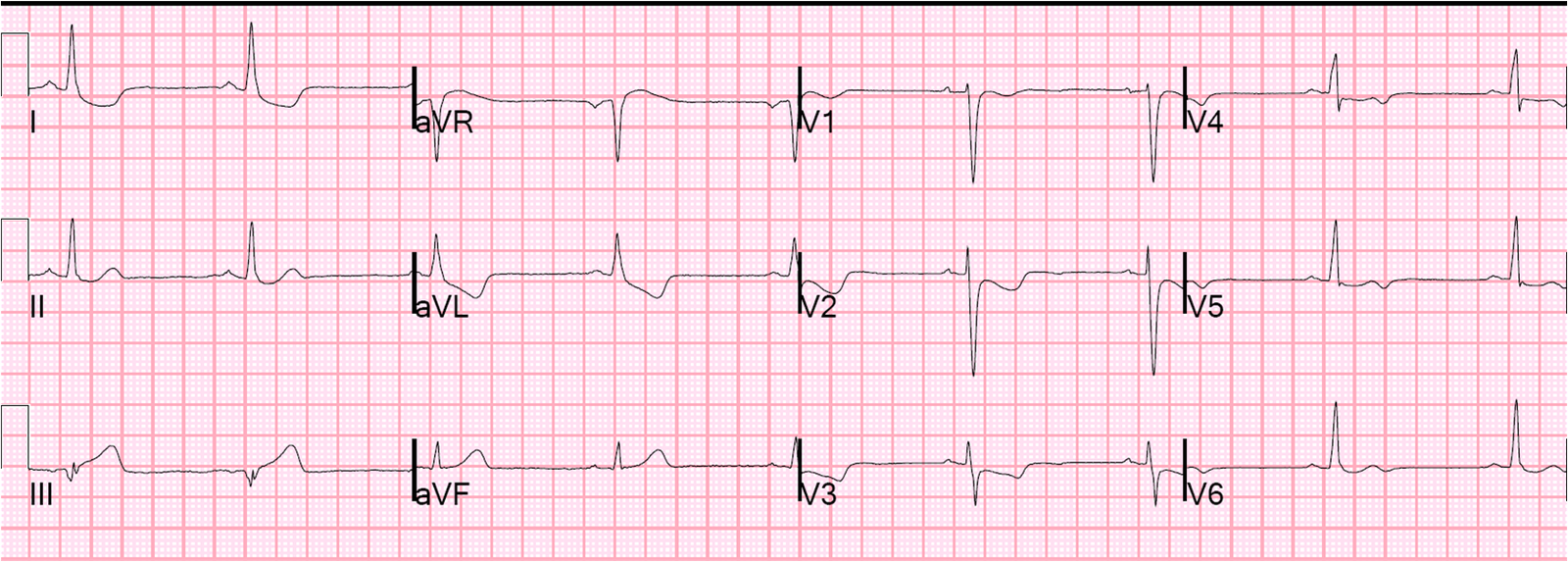
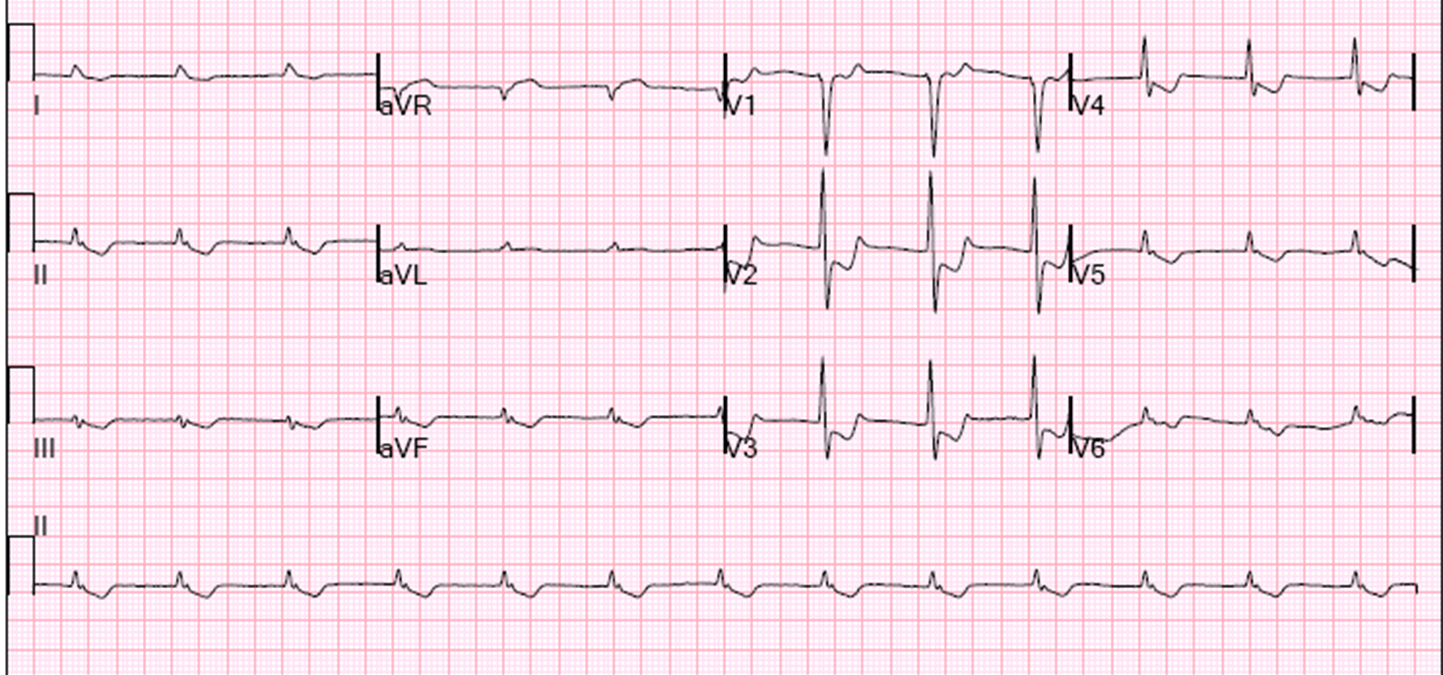
Here is a similar case involving right bundle branch block.
What is the normal QRS duration in LBBB?
In this study of consecutive patients with LBBB who were hospitalized and had an
echocardiogram, a QRS duration less than 170 ms (n = 262), vs. greater than 170 ms (n = 38), was associated with a significantly better ejection fraction (36% vs. 24%). Only 13% had a QRS duration greater than 170 ms, and only 1% had a duration greater than 190 ms.
Obviously, if you have a previous ECG for comparison, you can diagnose prolonged QRS in the setting of LBBB easily. But it is clear that if your patient with LBBB has a QRS duration greater than 190, then there is more going on.