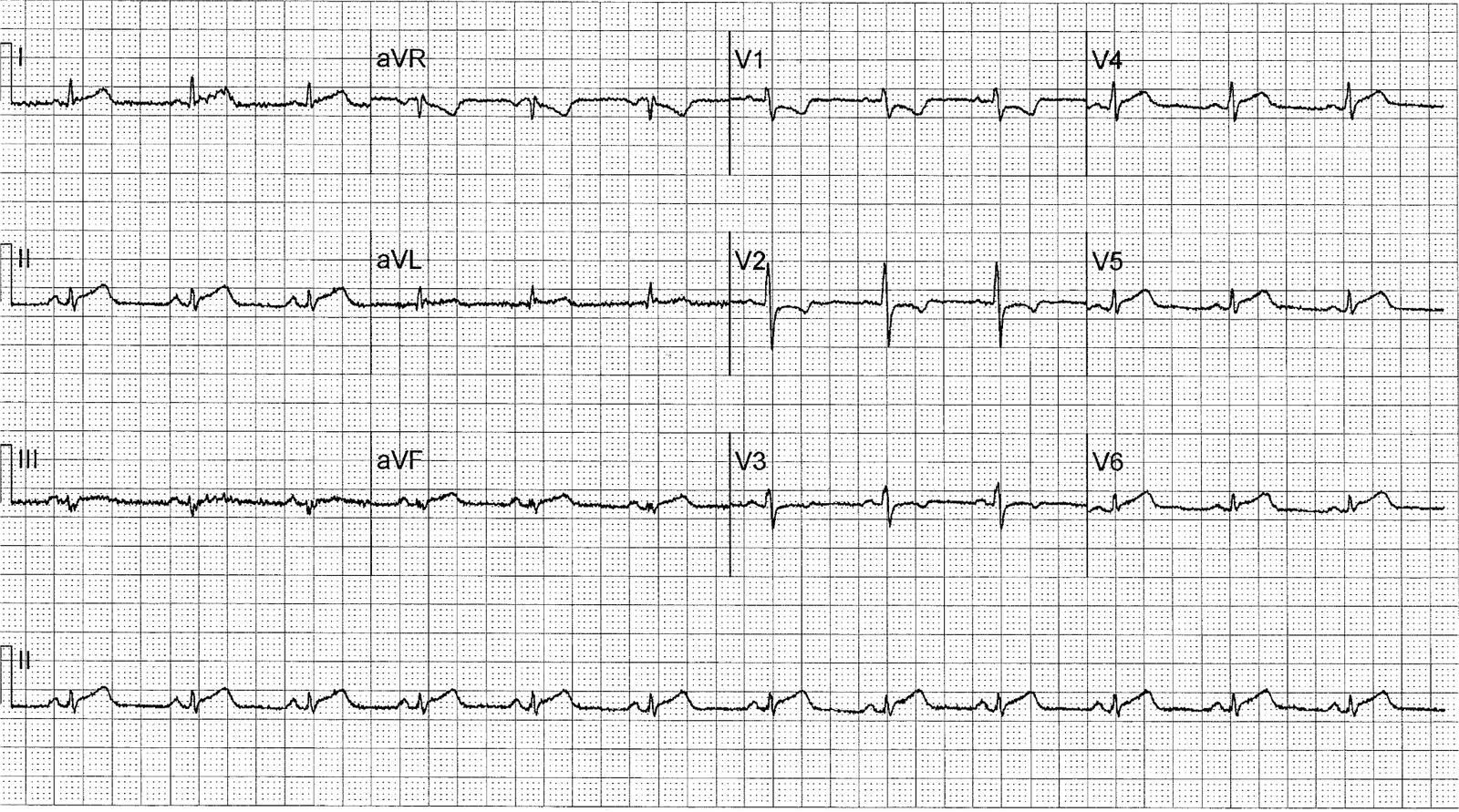
A 50 year old male presented to his physician’s office with “heartburn”. The physician recorded this ECG, interpreted it as normal, and sent the patient home on an antacid.
 |
| See explanation below. |
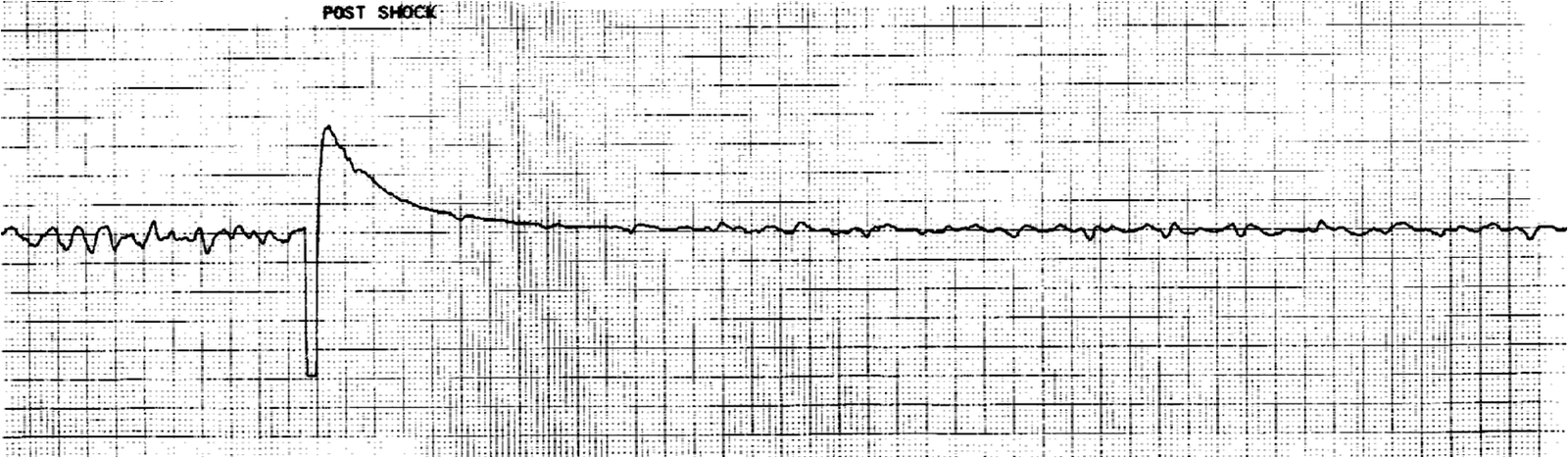
The patient went home and, in front of his wife, he collapsed. He underwent immediate CPR, was found to be in ventricular fibrillation, and was successfully resuscitated. I do not have the post-resuscitation ECG. He underwent coronary stenting (uncertain which artery). He underwent months of rehabilitation and was able to return to work part time.
Could this have been avoided?
1. A 50 year old with “heartburn” is a high risk complaint. There is no way to tell the difference between GI etiology of chest pain and MI. Therefore, even with a normal or non-diagnostic ECG, a 50 year old male patient should undergo serial ECGs and troponins and be admitted to a monitored bed until MI or ACS can be ruled out. This is obviously a very big topic in itself.
2. Did the ECG offer unseen hints? Yes
 |
|
|
These findings mandate that the patient at least get serial ECGs.
If these remain unchanged, then serial troponins. An emergency cardiac ultrasound could be very useful. And if definitive signs of ischemia develop, the immediate antithrombotic, antiplatelet, and anti-ischemic therapy is indicated, including an immediate angiogram, if symptoms and ECG findings do not resolve.
Lesson:
1. Chest pain should never be assumed to be from a GI source, even if you think the ECG is normal.
2. Ischemia on the ECG can be very subtle and is easily missed. Accurate interpretation requires a lot of skill, practice, and experience. Appreciation of these subtle ECG findings could have helped to avoid a cardiac arrest and its resulting permanent disability
3. Down-up biphasic T-waves are usually reciprocal to up-down biphasic T-waves in the opposing lead and are almost always ischemic
4. T-wave size must be evaluated in the context of QRS size.
Oertle, Paul