This ECG is from an article in the New England Journal on pericarditis.
Acute Pericarditis
N Engl J Med 2014; 371:2410-2416December 18, 2014DOI: 10.1056/NEJMcp1404070
A reader had read this post on ST depression in lead aVL in pericarditis vs. inferior STEMI.
He sent this ECG recorded from a patient with pericarditis and asked why there is ST depression in lead aVL:
 |
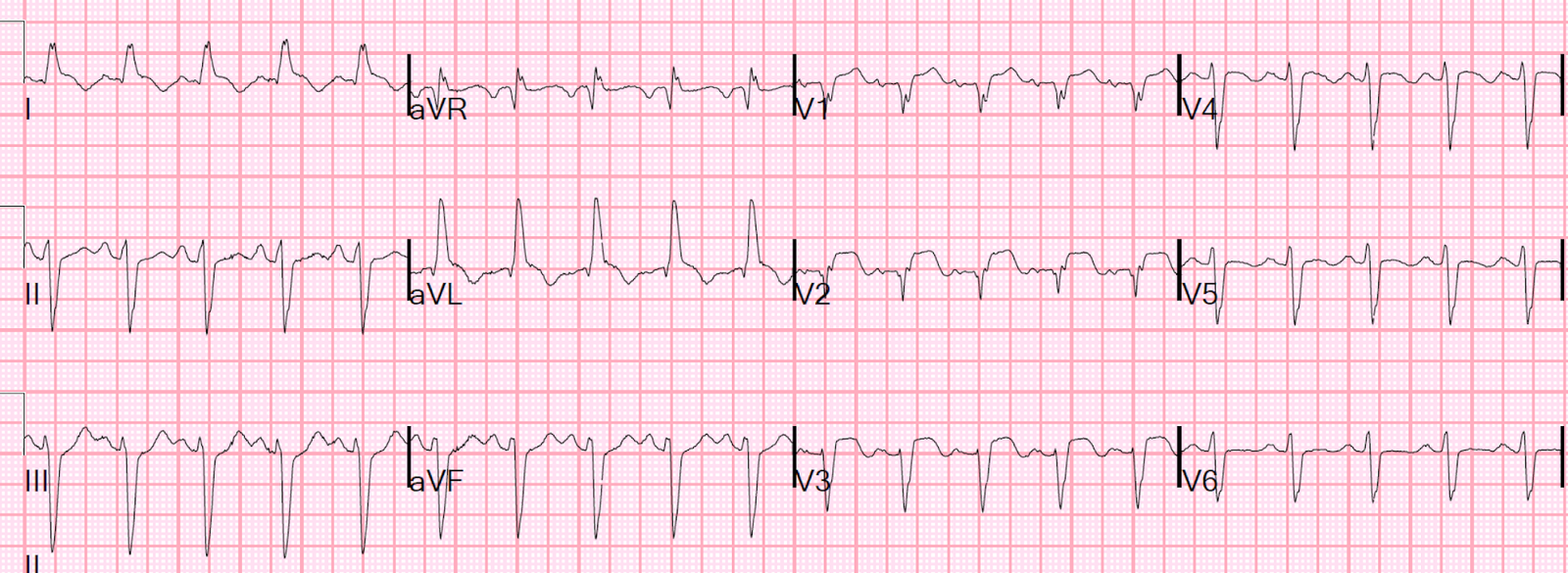
| There is sinus rhythm with diffuse ST elevation (especially in inferolateral leads, which is typical of pericarditis). There is diffuse PR depression and Spodick’s sign. There is a tiny amount of reciprocal ST depression in lead aVL. |
My answer to the reader is below:
As there are always exceptions to every rule, one must look at every ECG individually.
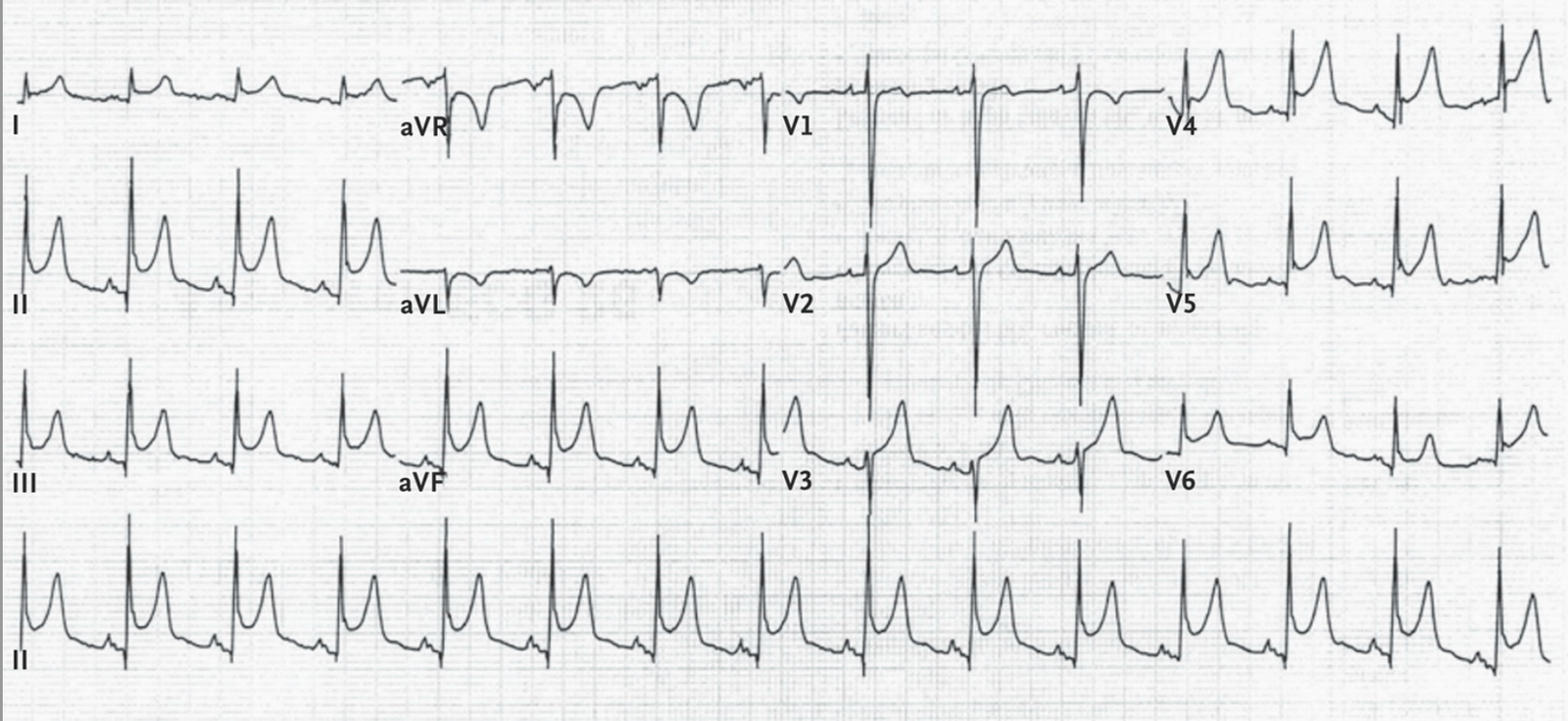
There is minimal ST depression in aVL, perhaps 0.5 mm.
Put that into the context of the whole ECG: there is very significant ST elevation in inferior leads. This is not subtle. When there is inferior MI with large ST elevation, there is nearly always marked reciprocal ST depression in aVL.
Proportional Analysis
Always interpret every ECG with proportional analysis. Everything should be proportional to everything else for any given diagnosis. In this case, you see very large inferior ST elevation, but only minimal (if any) reciprocal ST depression. The proportions do not make sense. This would be exceptionally unusual for inferior MI.
ST axis analysis
The ST elevation is higher in lead II (3mm) than lead III (2mm). This is also a pretty good ECG sign for pericarditis, as it implies the ST axis is closer to lead II than III, and less than 90 degrees. When there is ST depression in aVL, the ST axis must be to the right of lead II (greater than 90 degrees). Thus, the ST axis is between leads II and aVF (60-90 degrees). However, the fact that there is such minimal ST depression in lead aVL tells us that the ST axis is only BARELY greater than 60 degrees, perhaps 65 degrees. Thus, it is still very close to the normal axis for pericarditis (up to 60 degrees) and it is unusually leftward for inferior STEMI.
But, as I always say, you diagnose pericarditis at your peril, so always approach this with caution!
Steve Smith