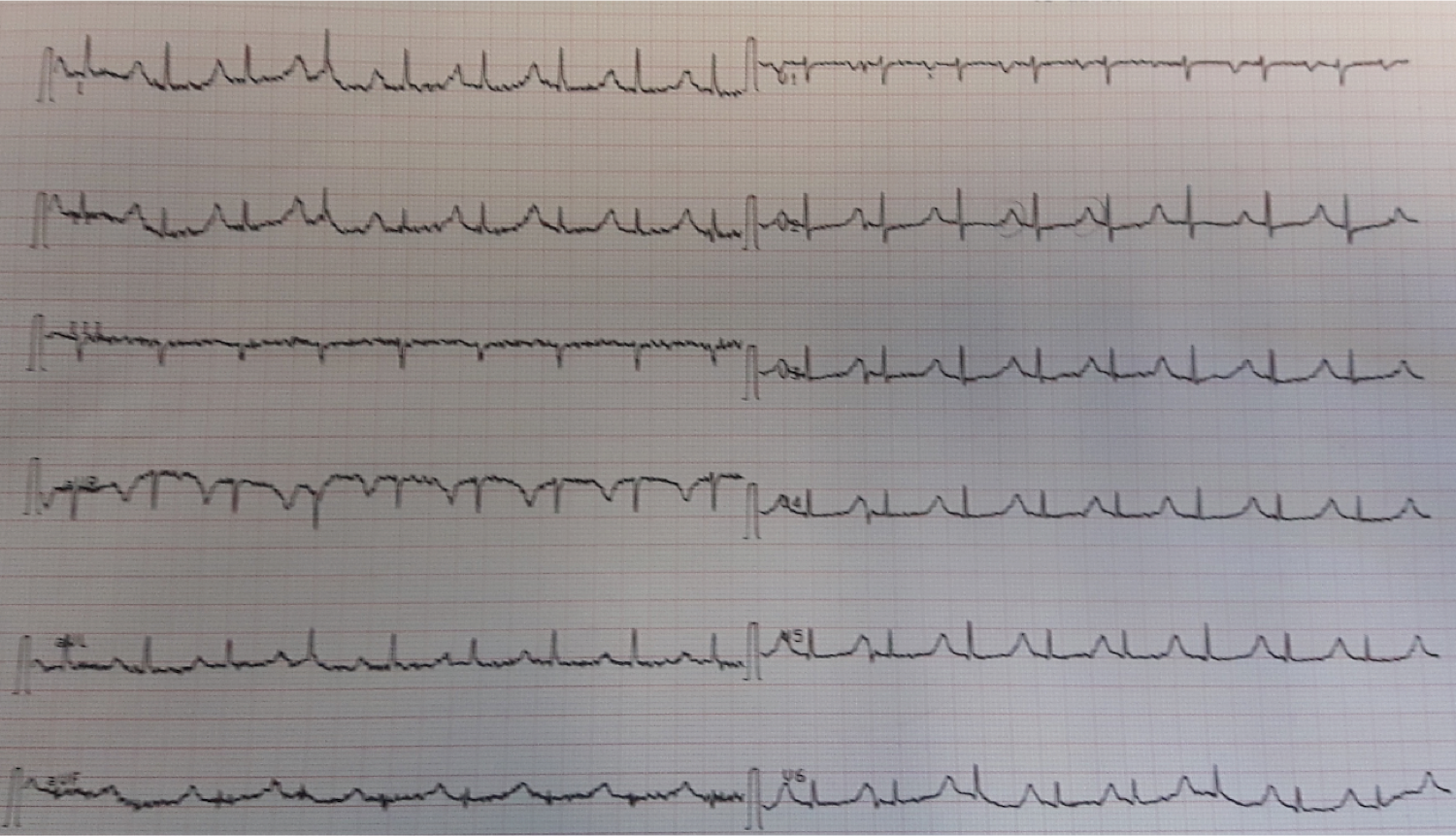
This late middle-aged male had sudden onset of chest pressure. Here is the prehospital ECG:
 |
| The rhythm is a bit hard to discern. It appears to be sinus with PACs. It is obviously an anterior (and lateral) STEMI. What other ominous finding is present? |
The cath lab was activated prehospital, and on arrival, the patient was in shock, with hypotension and an StO2 of 55% (this is a tissue oxygen saturation; normal is 75%. 55% represents shock no matter what the blood pressure). He denied SOB but immediate bedside ultrasound showed B-lines of pulmonary edema. Oxygen saturations were 94% on nasal cannula. BP was approximately 90 systolic.
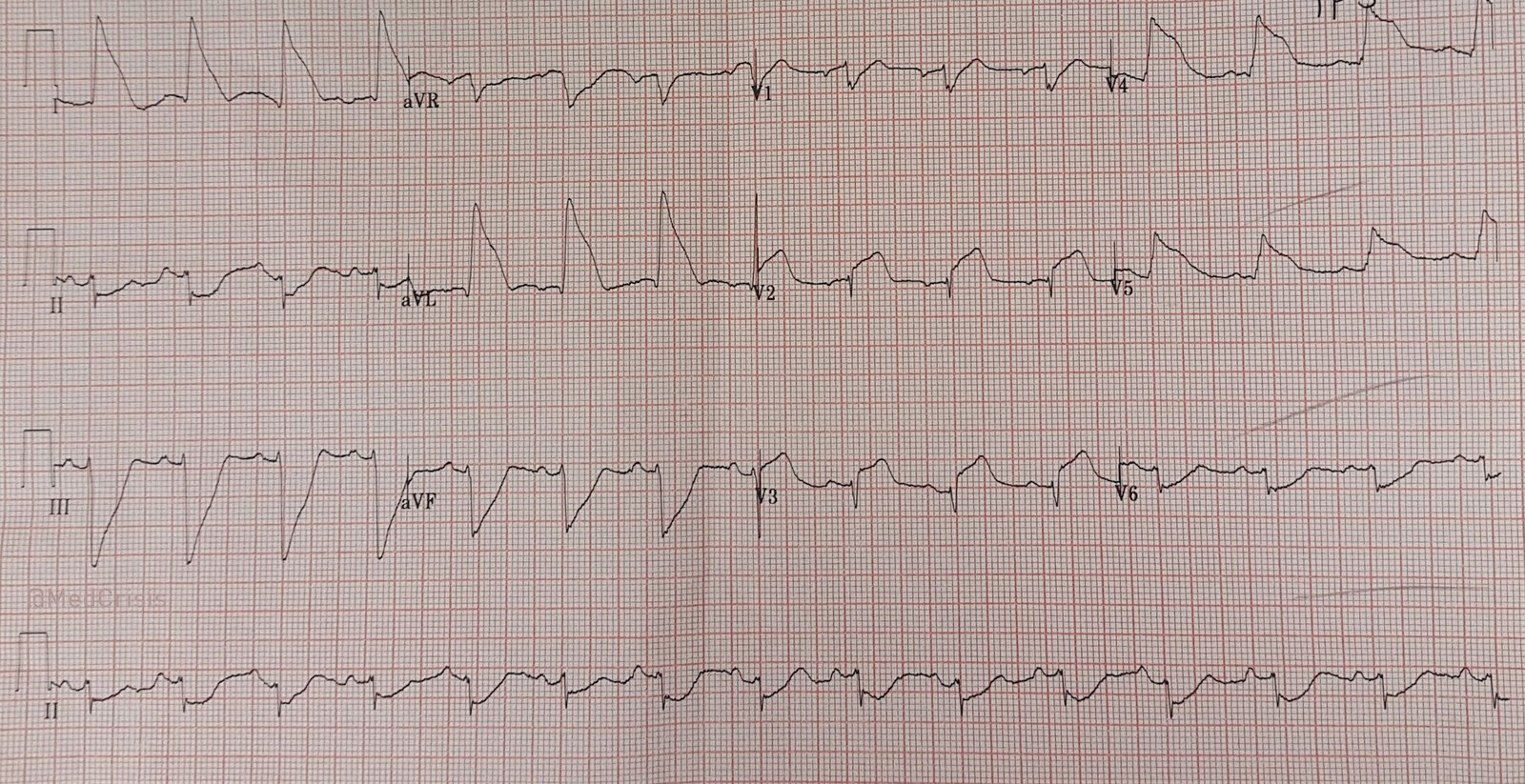
Here is the ED ECG:
 |
| Now there is atrial fibrillation with moderately rapid ventricular rate (126) There is huge ST elevation in V2-V4 and I and aVL, diagnostic of proximal LAD occlusion Here is the ominous finding: Right Bundle Branch Block (RBBB) + LAFB (left anterior fascicular block). |
I have seen a dozen cases of STEMI with RBBB and LAFB. All were close to death. This article by Widimsky illustrates the danger of this finding:
See these cases:
Chest Pain and Right Bundle Branch Block
Treatments:
1. Aspirin 325 mg
2. Ticagrelor 180 mg
3. Atorvastatin 80 mg (small studies support this)
4. Heparin bolus
5. Fluid challenge
6. Because cardiogenic shock is likely to get worse, even after reperfusion (because myocardial stunning lasts many days), we intubated the patient.
7. Vecuronium paralysis
8. Ketamine sedation (to avoid affecting hemodynamics)
9. K replacement.
10. Should have cardioverted, but did not
By this time, the cath team was ready.
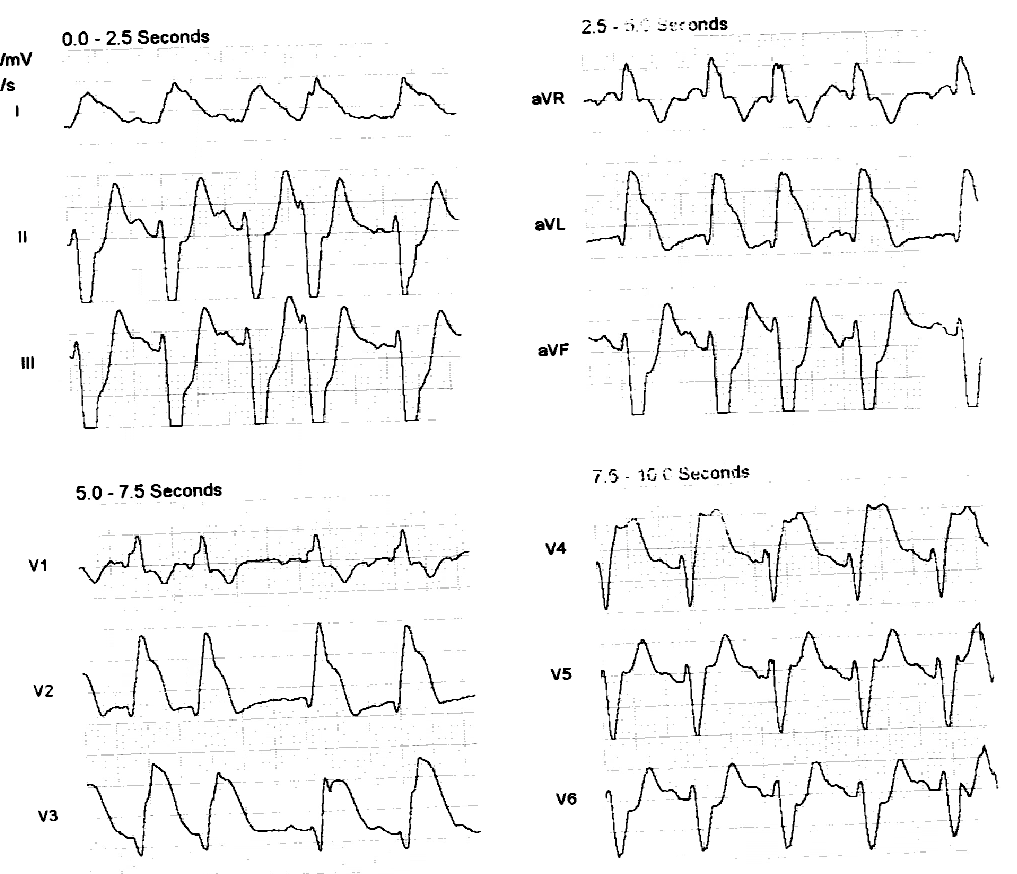
A proximal LAD thrombotic occlusion was opened. Here is the post-reperfusion ECG:
 |
| Sinus rhythm at a rate of 117. Uncertain if conversion was spontaneous, or done electrically in the cath lab RBBB and LAFB persist (not a good sign). ST elevation is greatly improved (a good sign), though still very elevated (not a good sign). There is terminal T-wave inversion, an early sign of reperfusion. |
A balloon pump was placed.
Here is the ECG the next day:
 |
| Q-waves and poor R-wave progression. RBBB and LAFB are gone. (A good sign). |
Highest troponin I was extremely high at 230 ng/mL at 10 hours after arrival.
Echo showed anterolateral wall motion abnormality and EF of 35%.
In spite of maximal supportive therapy, balloon pump, and persistently open arteries, the patient succumbed to cardiogenic shock 5 days later.
Learning Points:
1. Cardiogenic shock due to STEMI has very high mortality even if the artery is opened. The mortality is approximately 50%, and, surprisingly, use of a balloon pump appears to not change that terrible prognosis. (1)
2. RBBB and LAFB are signs of very severe ischemia
3. Although I know of no supporting literature, I almost always intubate STEMI patients with shock and pulmonary edema. Work of breathing may require 50% of cardiac output. Positive pressure ventilation and paralysis takes away all that work and all that excessive requirment for cardiac output.
1) Thiele H et al. Intra-aortic balloon counterpulsation in acute myocardial infarction complicated by cardiogenic shock (IABP-SHOCK II): final 12 month results of a randomised, open-label trial. Lancet. Volume 382, Issue 9905, 16–22 November 2013, Pages 1638–1645.