An elderly male called 911 for acute onset of shortness of breath and vomiting. EMS found him with a heart rate as high as 180 and hypoxic with O2 saturations in the 80’s.
A prehospital 12-lead was obtained:
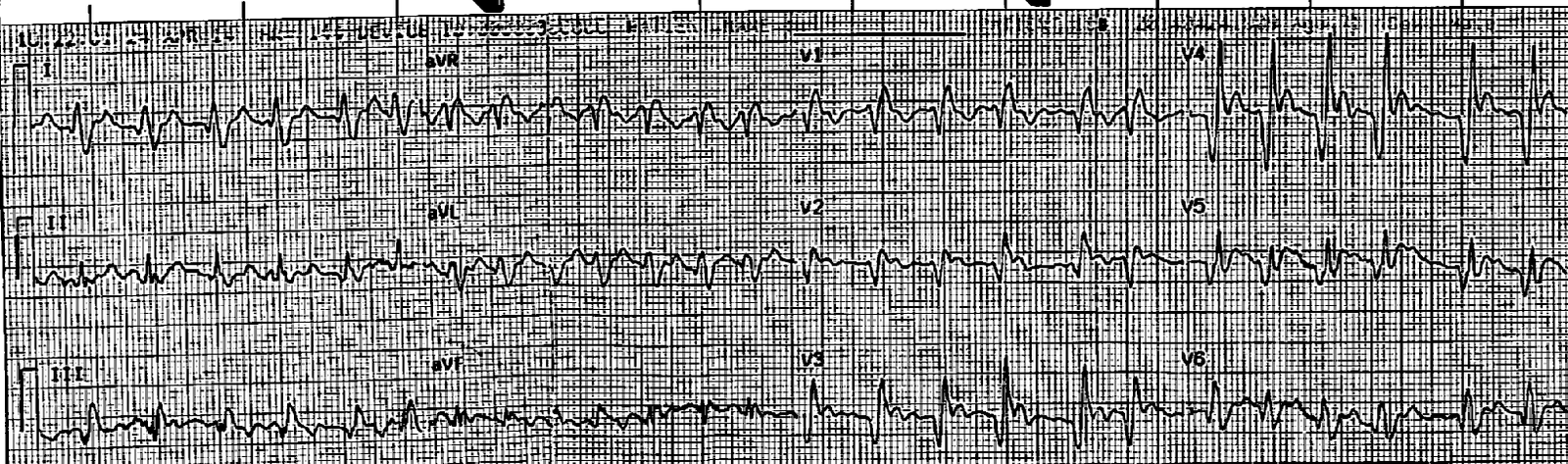 |
| There is atrial fibrillation (irregularly irregular, no P-waves) with a rapid ventricular response. There is right bundle branch block (RBBB). There is ST elevation in V2-V5. Is this acute STEMI?? |
|
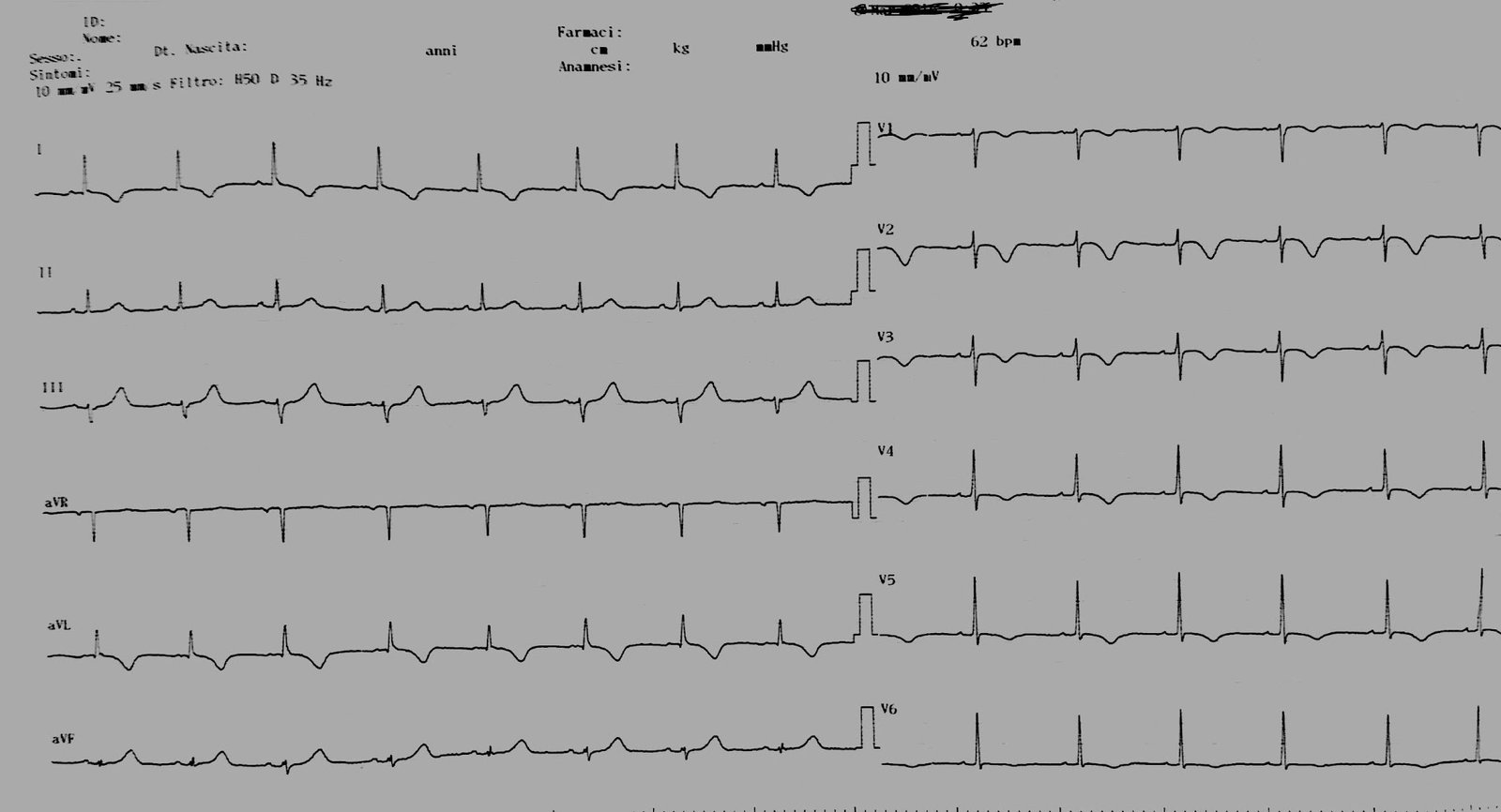
On arrival in the ED, the patient had this ECG recorded:
|
| Atrial fibrillation with RVR. ST Elevation in V2-V5. Is this acute STEMI? |

Note the well-formed Q-waves in the leads with ST elevation! This suggests old MI.
Comment: Old MI with persistent ST elevation, otherwise known as “LV aneurysm” morphology, usually has QS-waves (deep S-wave without a subsequent R-wave). But RBBB alters the sequence of ventricular activation such that the wave of depolarization ends by going to the right. Thus, an R-wave which would otherwise be absent is present in right precordial leads.
Normally, RBBB has rSR’. But with old infarction, the initial r-wave is obliterated and one is left with a QR. This can occur in acute STEMI with RBBB, but should raise the suspicion for LV aneurysm.
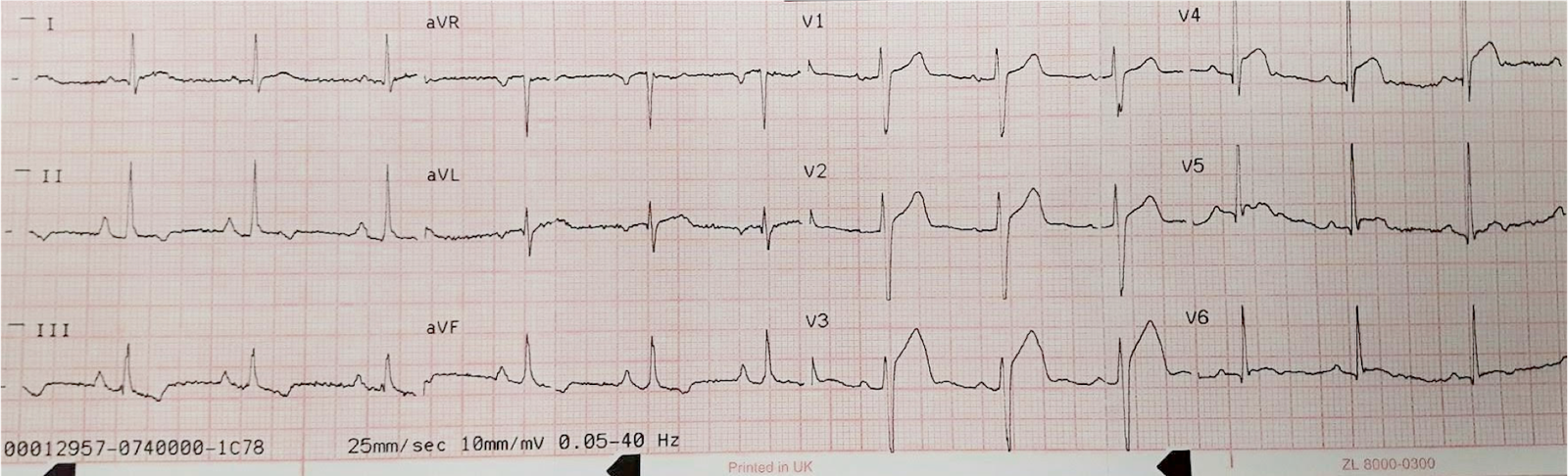
Let’s look at a second instructive case in which the patient alternated between RBBB and normal conduction:
 |
| Note classic anterior LV aneurysm morphology (QS-waves in V1-V3 with ST elevation). There is ST elevation, but the T/QRS ratio is less than 0.36 in all of leads V1-V4, indicating that it is not acute STEMI. I derived and validated this rule. |
The patient with the above ECG presented twice with chest pain and RBBB, with this ECG:
 |
| There is ST elevation in V1-V4 without the deep QS-waves.
But there is RBBB. The patient has an intermittent, possibly rate-related, RBBB. |
Back to the first case:
The patient’s record was available. It revealed that the patient had a known LV aneurysm with this ECG 4 months prior:
 |
| Same, except there is a slower ventricular response. |
The Previous Echo
–Left ventricular ejection fraction is 29%
–Decreased left ventricular systolic performance, severe.
–Regional wall motion abnormality-distal septum anterior and apex diastolic
distortion with dyskinesis (aneurysm) large.
–Regional wall motion abnormality-distal inferior wall akinetic (part of LV
aneurysm)
–No evidence for left ventricular thrombus
Further history revealed that he had nausea and vomiting earlier in the day and that he might be dehydrated. His inferior vena cava was “collapsing” on ultrasound (this is not always reliable). On the other hand, there were B-lines and reported pulmonary edema on CXR. The ejection fraction on bedside ultrasound was consistent with the previous echo.
On history, he claimed to have been taking his chronic AV nodal blockers for atrial fib.
Exam revealed lower extremity cellulitis, but there was no fever.
Thus, the clinical picture was confusing. A Diltiazem drip was started, with some improvement but a fall in blood pressure.
The ultimate interpretation of the data was that some dehydration and sepsis had led to high adrenergic state and rapid ventricular response, which led to decreased ventricular filling and, paradoxically, pulmonary edema.
He improved greatly with both fluids and diltiazem.
There was no acute coronary syndrome.
Troponin I peaked at 0.829 ng/mL (consistent with demand ischemia and type 2 MI).
Learning Points:
1. LV Aneurysm can mimic acute STEMI
2. RBBB distorts the ECG of LV aneurysm morphology, further mimicking acute STEMI.
3. Most Atrial Fib with RVR is due to acute disease superimposed upon chronic atrial fib
4. Management of fluid status and rate control in chronic atrial fib can be very complex.