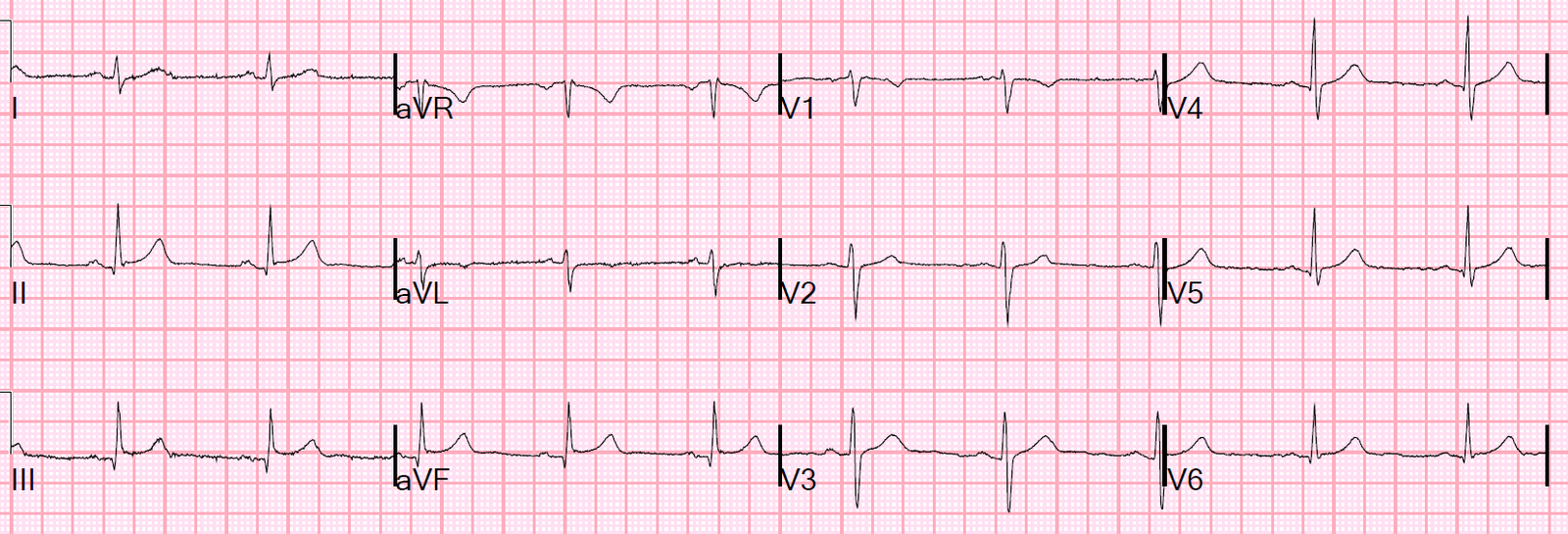
A 60-something male called 911 for chest pain of less than one hour duration. He arrived in the ED pain free and had this ECG recorded:
 |
| What to you think? |
There are hyperacute T-waves in V2-V4, but the patient was pain free. I did wonder if he had had a prehospital ECG recorded, and what it showed.
This was 10 years ago, just when we had started doing prehospital 12-lead ECGs. I was not even certain that one had been recorded, but if it was, I wanted to see it.
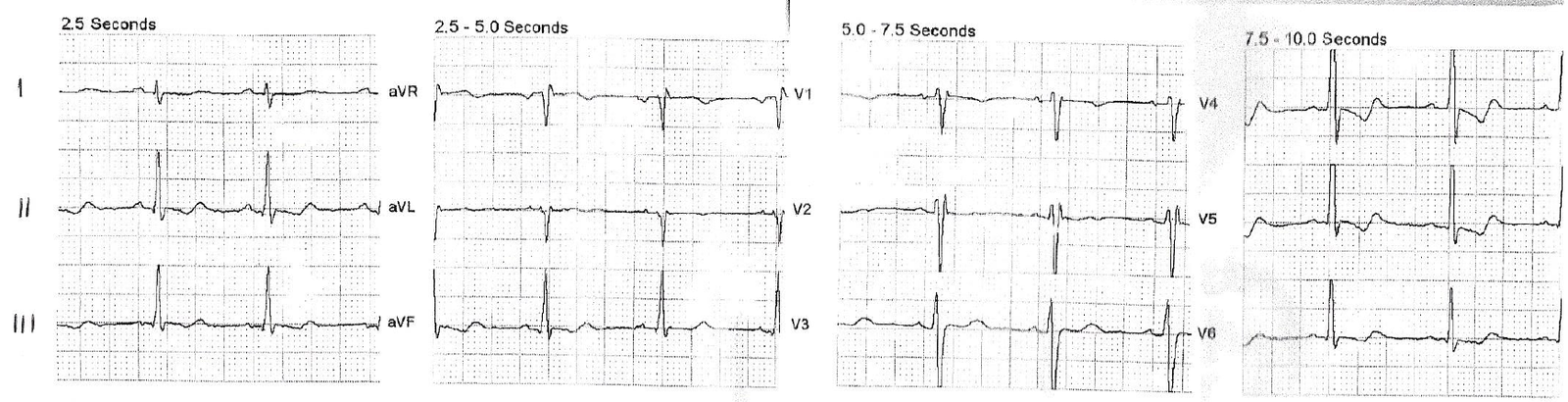
I had to look around for it, and here is what I found:
 |
| Pretty amazing, huh? |
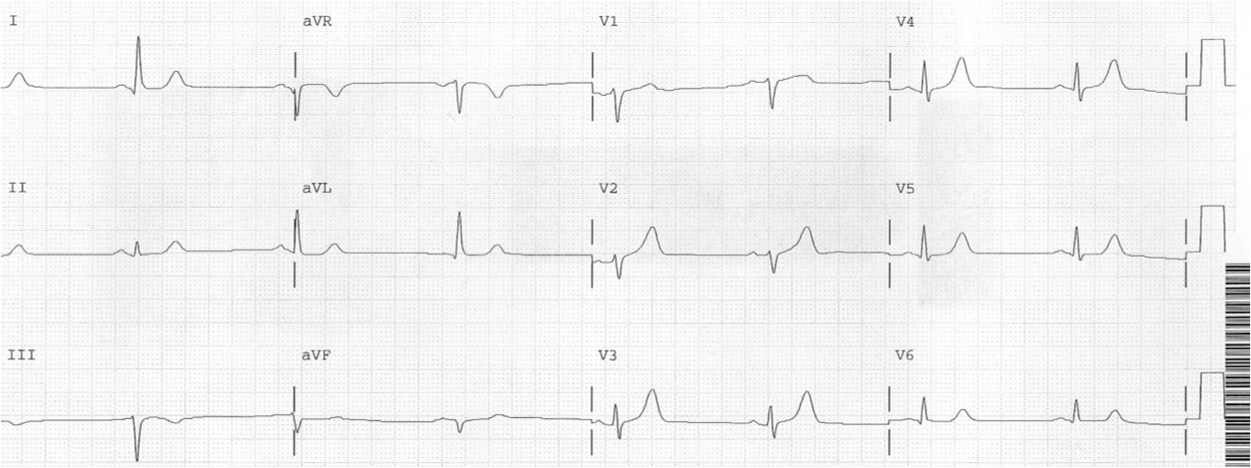
Here I have circled the computer algorithm interpretation, just so you don’t miss it:
 |
| Early Repolarization??? Notice STE is both precordial and in I/aVL. |
He was taken to the cath lab and there was a fresh thrombus in the proximal LAD with 80% stenosis.
Serial troponins were all undetectable (these are less sensitive than today, but as I pointed out in my last post, the initial troponin in STEMI, even with high sensitivity troponin, can be below the level of detection.
Here is another case where the physicians did not seek out the prehospital ECG and it led to loss of myocardium, but in this case for missing the evolution. The initial troponin was below the level of detection.
Learning Points:
1. In spontaneously reperfused “Transient STEMI,” hyperacute T-waves may still be present after resolution of pain and resolution of ST segments.
I say: “you get hyperacute T-waves on the way up (as ST segments are on the way up, shortly after occlusion) and on the way down (after ST segments have normalized, shortly after reperfusion)
2. The Initial troponin is often undetectable in STEMI
3. Serial troponins may be all negative in transient STEMI
4. Always look for and examine the prehospital ECG.