A 60-something male with CAD w prior stenting, prior LV thrombus, ischemic cardiomyopathy, HFrEF with his last ejection fraction (EF) at 41%, and prior CVA was brought by medics with chest pain that began two hours prior and feels like his prior MI. Non radiating. On arrival, he states that the pain has resolved.
He received 324 of ASA prior to transport. Prehospital vitals were notable for severe hypotension, bradycardia to the 50s, and inability to obtain reliable oxygen saturation, glucose 168.
In the ED, the BP was 56/46 and the patient was confused but able to follow commands. O2 saturation on oxygen was 97%.
Bedside ultrasound showed EF of approximately 10%, with only one myocardial wall demonstrating any wall motion: the septum. You can see that the RV is also not enlarged.
He also had pulmonary edema (B lines on bedside ultrasound)
= = =
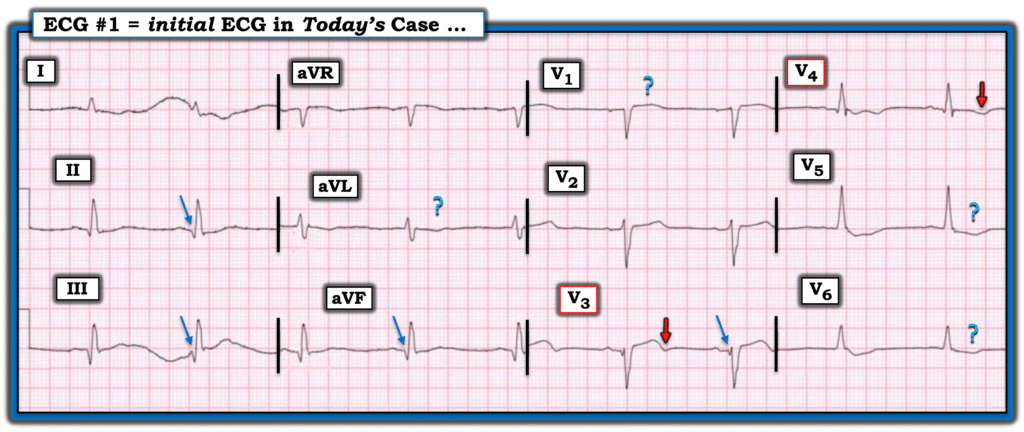
Here is his initial ECG:
What do you think?
There is minimal STE in V2, V3, with a resolving hyperacute T-wave in V3 (T-wave turning down). There is minimal but significant STE in V1, with STD in V5,6. This is very concerning for precordial swirl. To me, the ECG represents reperfusing LAD, which corresponds to the shock and resolved chest pain.
Here is the Queen of Hearts interpretation, applied later for this post (not for clinical care):
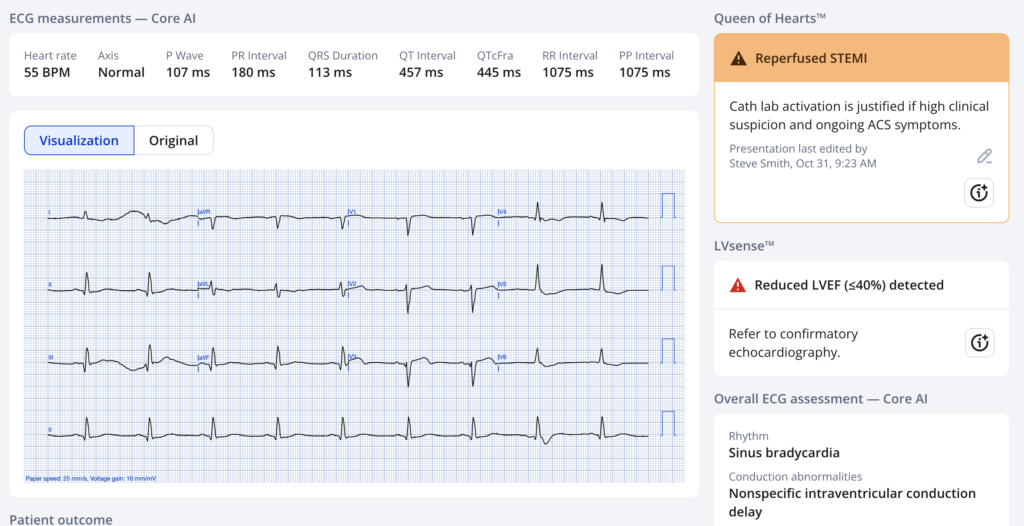
The Queen of Hearts has the same impression that I do. “Cath lab activation is justified if high clinical suspicion and ongoing ACS symptoms.”
There is very high suspicion and ongoing shock. Acute Cardiogenic shock with acute LV pump failure must be considered to be due to acute OMI no matter the ECG findings and no matter the disappearance of chest pain.
Thus, the cath lab was activated for chest pain and cardiogenic shock.
There was a brief arrest with ROSC. He was intubated.
Lactate returned at 4.2 mEq/L, first hs troponin I at 7 ng/L.
DO NOT TRUST THE FIRST TROPONIN!!
Angiographic findings:
1. Left main: no relevant stenosis, large.
2. LAD: chronic in-stent occlusion after the first septal perforator. The distal LAD is supplied by left-to-left collaterals.
3. LCX: (probably acute thrombotic) proximal occlusion. It supplies a large OM1 that also supplies the LAD and distal RCA/RPDA/RPLA with collaterals.
4. RCA: chronic in-stent occlusion. The distal RCA/RPDA/RPLA are supplied by left-to-right collaterals and right-to-right collaterals.
Thus, the only myocardial wall being supplied is the septum, since the LAD is occluded AFTER the first septal perforator. The circumflex territory is GONE, as is the LAD territory because it is supplied by left to left collaterals. The RCA territory is GONE because it is supplied by left to right collaterals.
This all explains the pump failure and that the only wall motion working is the septum.
Impression:
1. Profound cardiogenic shock.
2. Severe three vessel coronary artery disease with a chronic (instent) LAD occlusion, chronic (in-stent) RCA occlusion and (probably acute) proximal LCX occlusion.
3. Successful LCX recanalization and stenting with a drug eluting stent.
4. Intra-aortic balloon pump insertion.
5. Right heart catheter insertion (at 60 cm).
Formal Echocardiogram:
Decreased left ventricular systolic performance, very severe
Regional wall motion abnormality-distal septum anterior and apex, akinetic, large
Regional wall motion abnormality-distal septum anterior and apex diastolic distortion with dyskinesis (aneurysm) large, probable
Impella was placed
Peak hs Troponin I > 60,000 ng/L
Ultimately, the patient died in spite of excellent care. Such is the outcome of almost 50% of patients in cardiogenic shock from acute coronary occlusion.
= = =
======================================
MY Comment, by KEN GRAUER, MD (4/6/2026):
- NOTE: At the time I am writing My Comment — I have only seen today’s initial ECG. I have not see a prior (baseline) ECG, nor have I seen any repeat tracings — which of course is a “realistic” scenario — since clinicians at the bedside often have to initiate clinical decision-making on the basis of a single initial tracing.
= = =
For me — interpretation of today’s initial ECG depends greatly on the history. If this ECG was from a patient who had an MI in the past — but who had done well for years, was currently asymptomatic, and came in now for “routine follow-up” — then I would suspect that the ECG picture we see in Figure-1 represented old disease and nothing acute.
However — that was not the clinical presentation for today’s case. Instead, essential components of today’s case include the following:
- The patient has known severe coronary disease — with prior stenting and resultant ischemic cardiomyopathy;
- He presents now with new CP (Chest Pain) that began ~2 hours before ECG #1 was recorded;
- His CP has now resolved!
- At the time ECG #1 was recorded — this patient was hypotensive with pulmonary edema — presumably in cardiogenic shock.
= = =
How to Interpret Today’s Initial ECG?
My “Descriptive Analysis” of the findings that we see in ECG #1 will be the same regardless of whether this patient is asymptomatic or in cardiogenic shock from an acute event, albeit now without any CP.
- The rhythm is sinus bradycardia at a rate slightly less than 60/minute. Intervals (PR, QRS, QTc) and the axis are normal. No chamber enlargement.
- The small but surprisingly wide Q waves in the inferior leads suggest there has been inferior MI at some point in time (BLUE arrows). There is no ST segment deviation in these inferior leads — and no more than very shallow T wave inversion in lead aVL of uncertain significance.
- The 2 leads that caught my “eye” — are leads V3 and V4. The Q wave in lead V3 is not normal (with a smaller Q wave also seen in neighboring lead V4). Septal Q waves are not this anterior — especially in the absence of any septal q waves in lateral chest leads V5,V6.
- The ST segment in lead V3 is straightened (albeit no more than minimally elevated) — with terminal T wave inversion.
- There is shallow T wave inversion in lead V4.
- I added question marks to the ST-T waves in leads V1,V5,V6 — as I was not sure what to make of these findings.
BOTTOM Line: The clinical scenario of known severe coronary disease — with this patient now presenting for new acute CP in cardiogenic shock clearly suggests extensive acute infarction. Given these clinical implications — complete resolution now of this patient’s CP strongly suggests spontaneous reperfusion of the “culprit” artery, which presumably is the LAD.
- “Pseudo-normalization of the ECG may be seen if a tracing is recorded in between the stage of acute ST elevation — on the way toward developing reperfusion T waves (suggested in ECG #1 by the RED arrows — and perhaps as well by the question mark ST-T wave depression in leads aVL,V5,V6).
- Finding a prior (baseline) ECG on this patient and/or repeating this ECG within the next few minutes will probably yield a definitive answer. That said — regardless, cardiac cath is clearly indicated as soon as this is feasible to define the anatomy and hopefully find a “culprit” amenable to lifesaving PCI.
= = =
Figure-1: I’ve labeled the initial ECG in today’s case.