A 40-something woman with Chest Pain of 20 minutes duration called 911.
It started while at rest and she describes it as crushing pain radiating
to the left arm. She has a history of HTN for which she takes
Lisinopril. Denies any other medical history.
She
appears well but in obvious pain. She was diaphoretic but pink
and warm. BP remained 150-160 systolic throughout care.
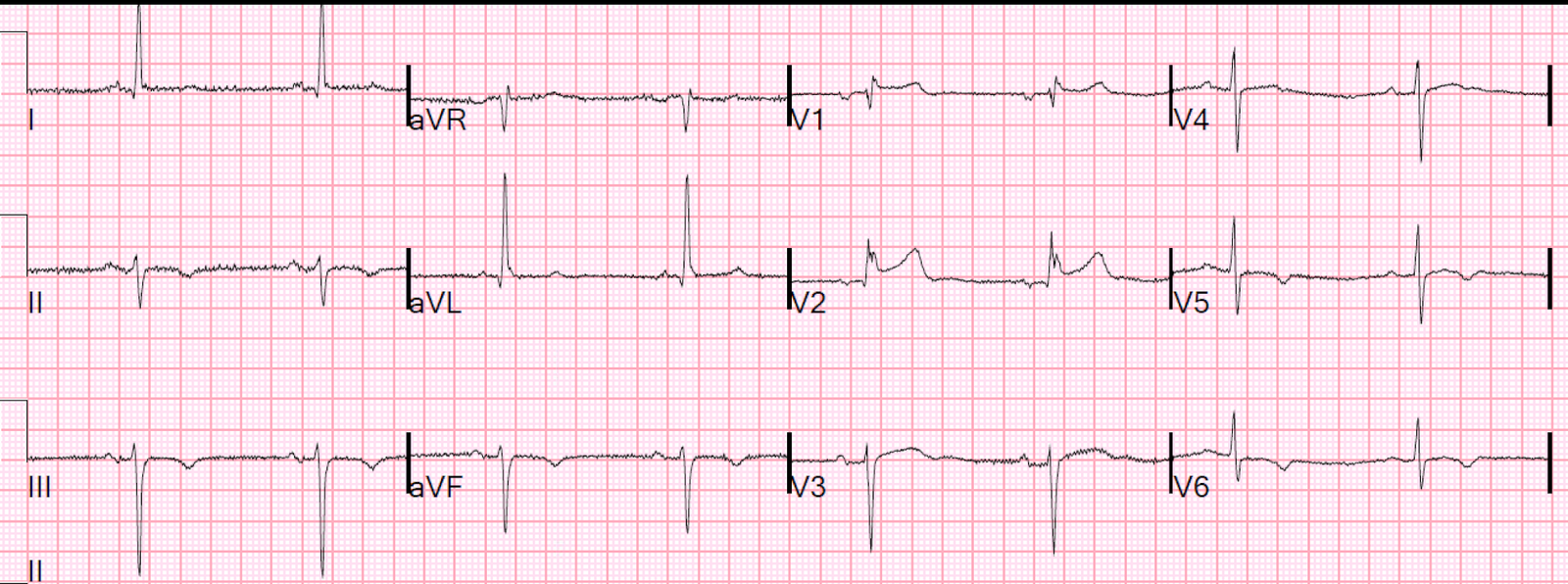
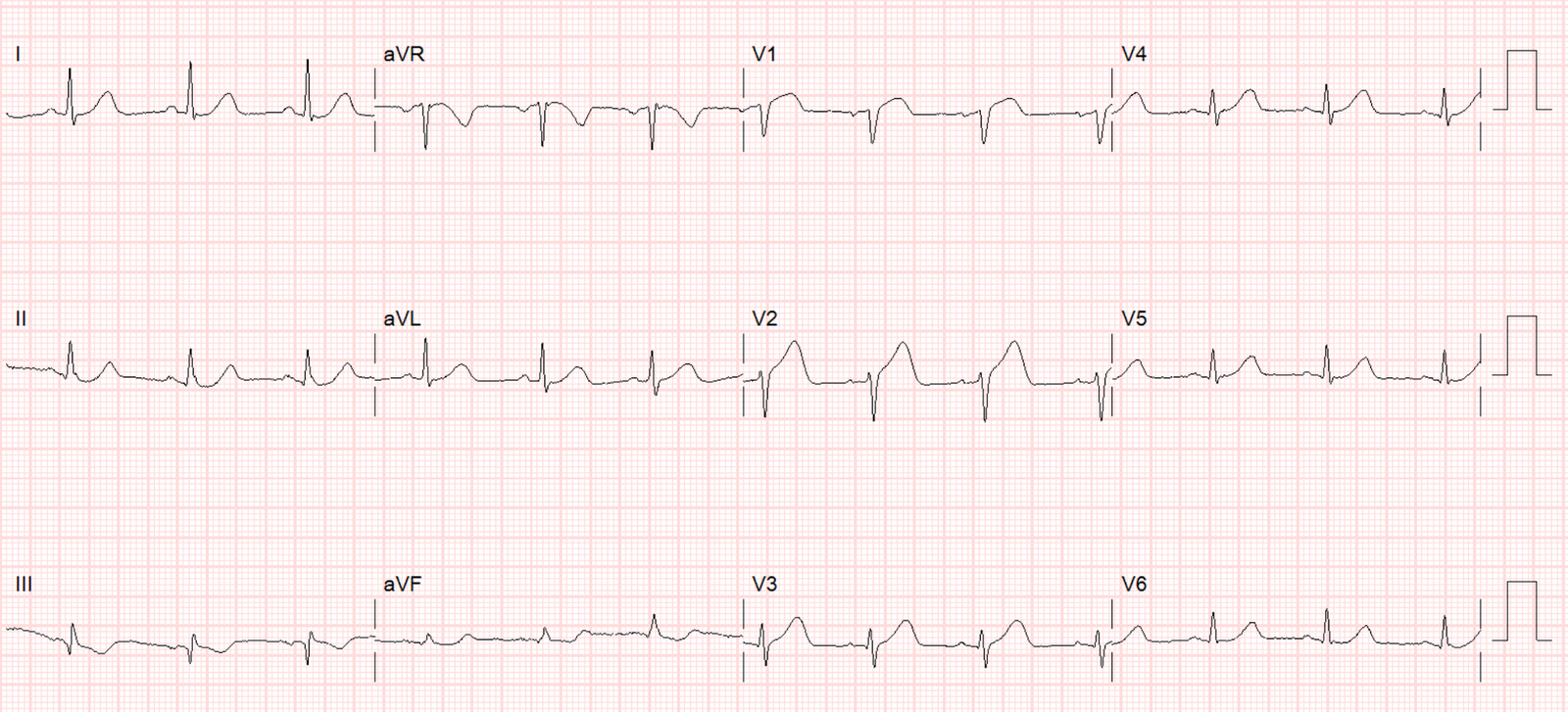
This prehospital ECG was
obtained.
 |
| There are very suspicious ST elevation and T-waves in V2, but without 2 consecutive leads with STE of greater than or equal to 1.5 mm, it does not meet STEMI criteria. |
The medic used the formula for differentiating LAD occlusion from Precordial Normal Variant ST Elevation (also commonly referred to as “Early Repolarization”)
With a computerized QTc of 430, the formula value was 24.94. Since this is greater than 23.4, the ECG represents LAD occlusion with a high degree of certainty.
Because of this, they bypassed the nearest hospital and transported the patient to the nearest STEMI receiving facility, which has PCI capabilities.
On the way, they recorded 3 more ECGs:
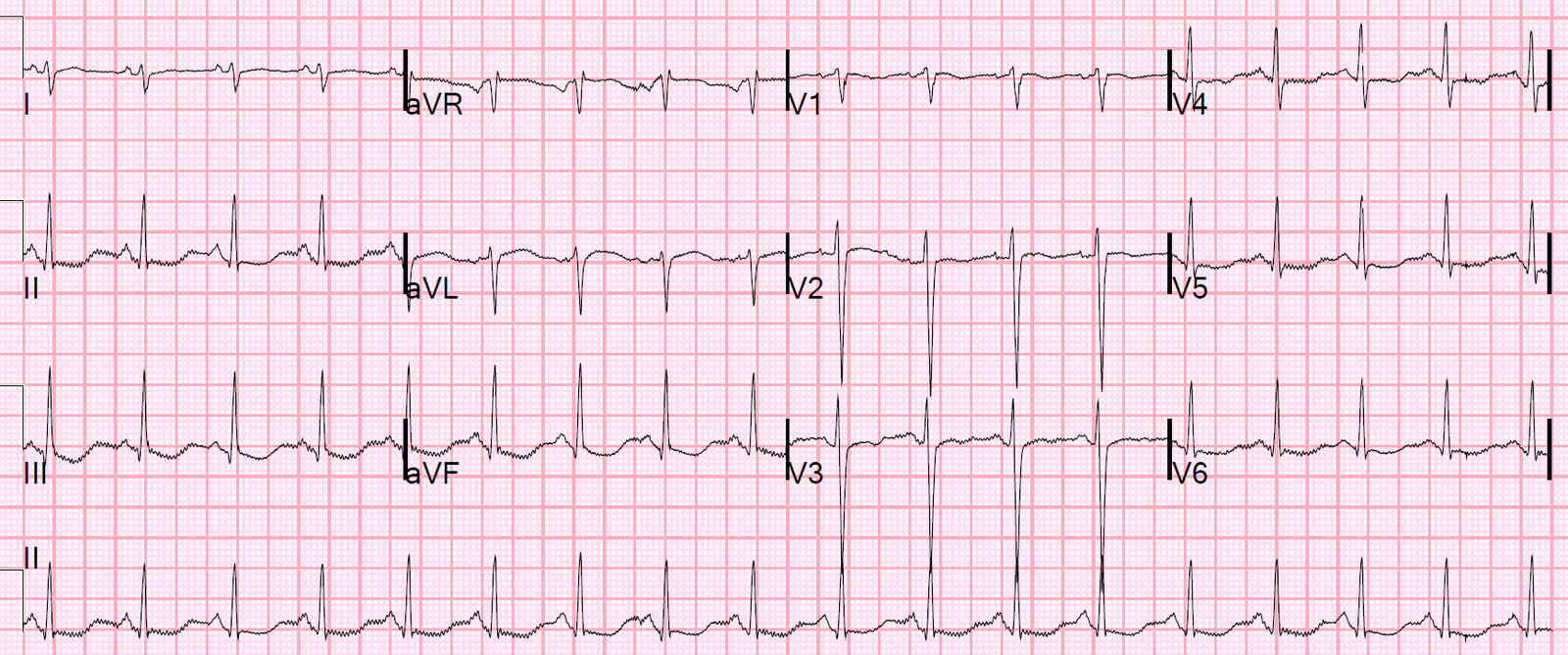
Time 5 minutes
 |
| No major change
This one was transmitted to the receiving facility, with request to activate the cath lab. |
When the emergency physician would not activate, the medic took things into his own hands and contacted the cardiologist himself. As soon as the cardiologist saw the ECG, he activated the cath lab.
2 more ECGs were recorded en route:
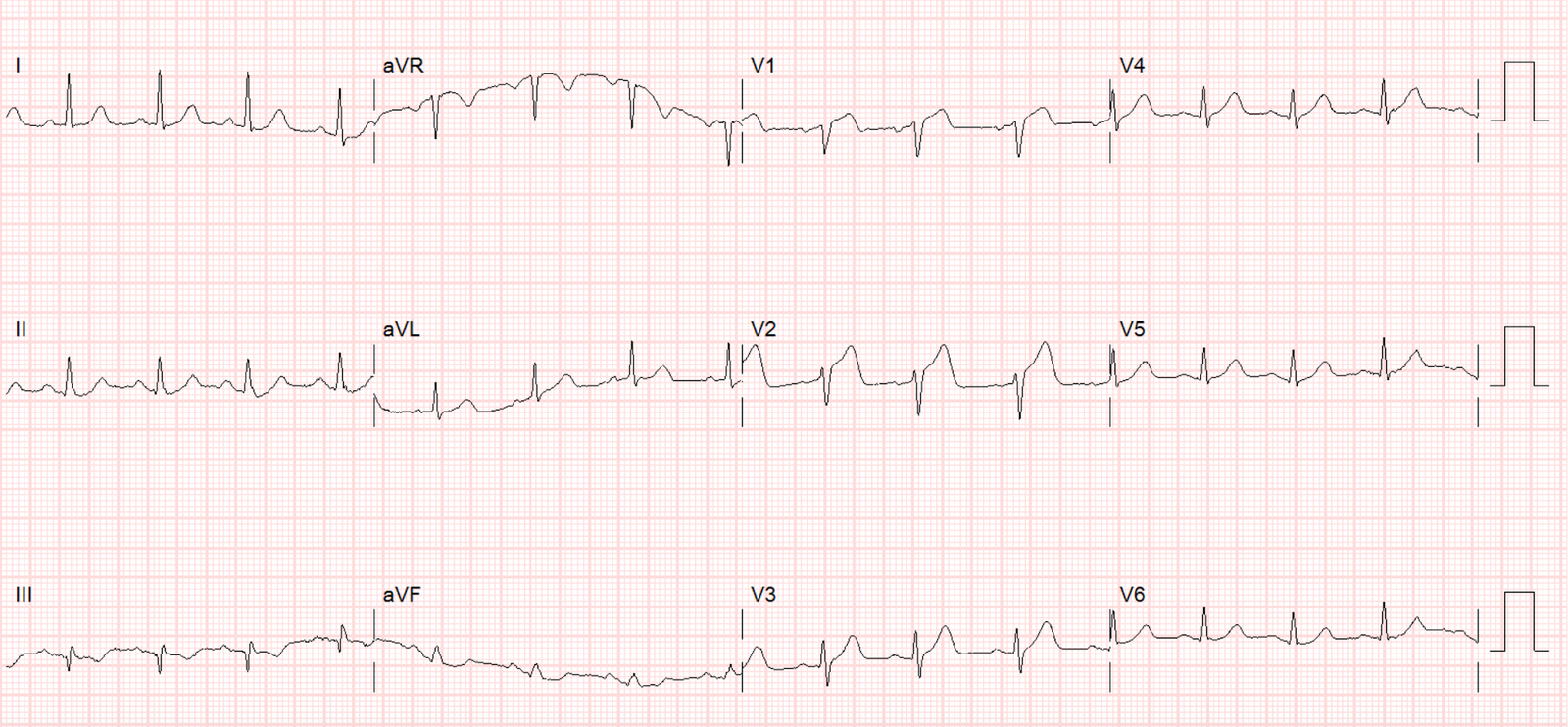
Time 30 minutes
 |
| Still no major change |
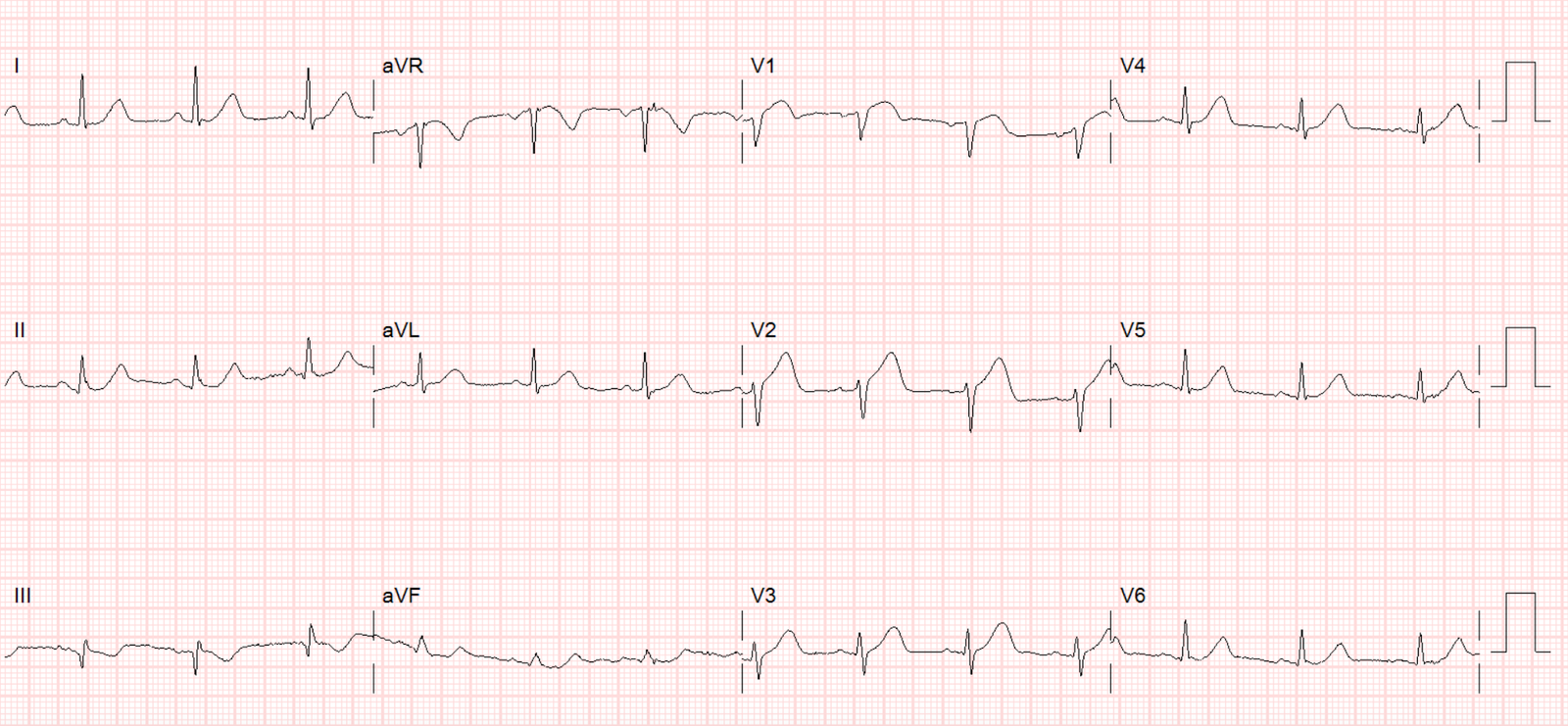
Time 33 minutes
 |
| Still no major change |
The patient bypassed the ED and went directly to angiogram:
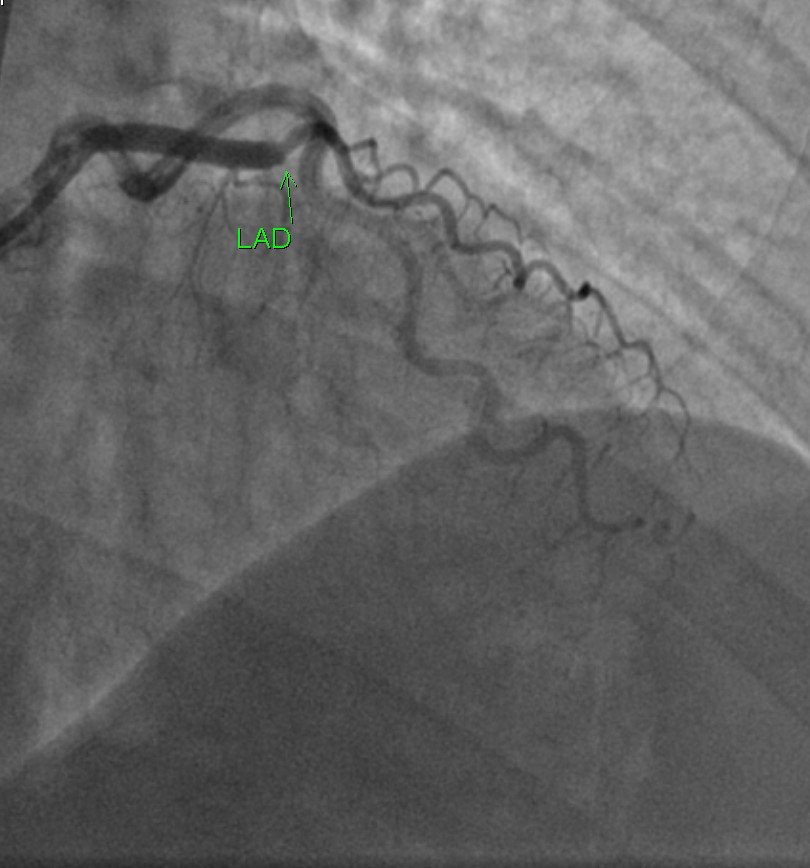 |
| There is a cutoff of the LAD (100% occlusion) The location is, to my eye, immediately after the takeoff of the first diagonal. (This is my interpretation of the angiogram and angiography is not my expertise — I might have the exact location wrong) |
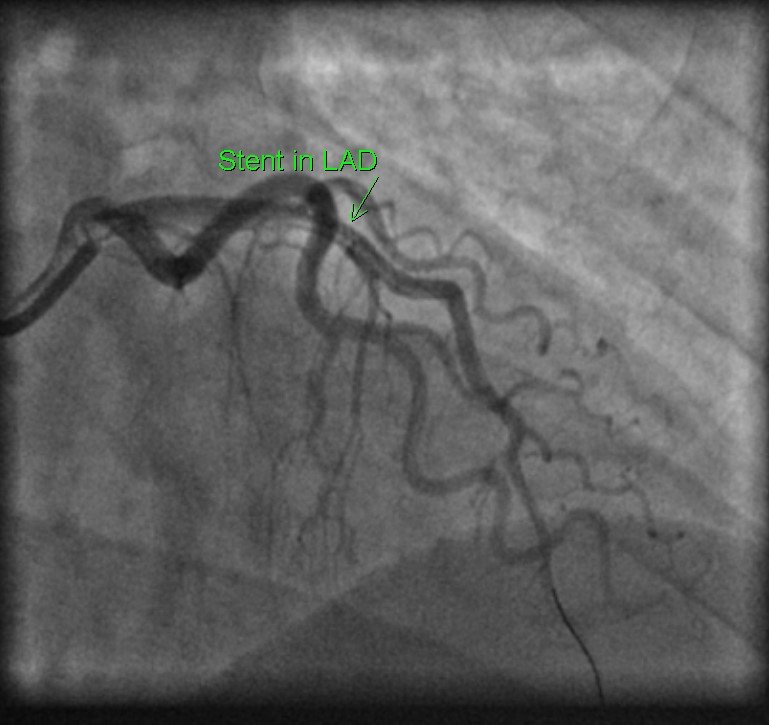 |
| After stenting, there is good flow in the LAD |
Learning Point
Subtle LAD coronary occlusion can be diagnosed by medics, especially with use of the formula. It may greatly aid in triaging patients to the appropriate hospital and aid in improving door to balloon time.