I was sent this ECG by a resident from elsewhere, with the following information:
“Young previously healthy man with several 10-20 minute episodes of chest pain over the past few hours, asymptomatic on presentation and during this ECG.”
“What do you think?”
 |
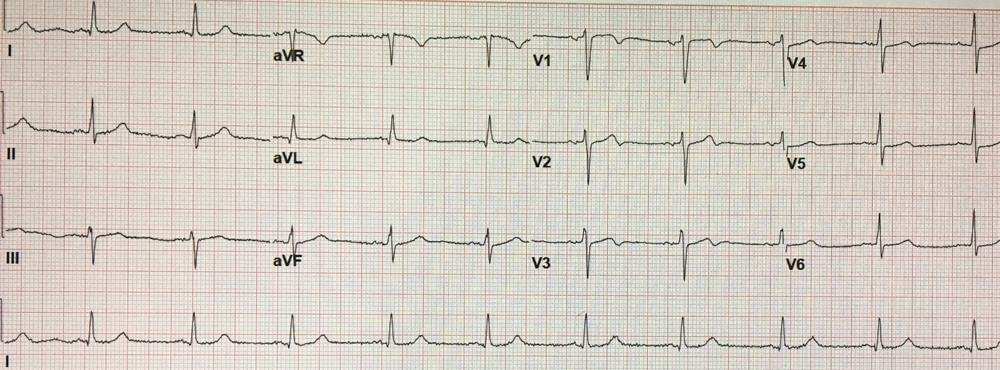
| There are Q-waves in V2 and aVL. The T-wave in V2 is too large for this Q to be due to old MI. There is minimal STE in aVL and a proportionally large T-wave, with a reciprocally large T-wave in lead III and a biphasic down-up T-wave in aVF.
There is some STE in V2 and V3, but this cannot be called normal variant because there is a Q-wave in V2 and poor R-wave progression. |
Here is my response:
“Old MI with superimposed LAD or First Diagonal acute ischemia. Q-wave in V2, aVL suggest old MI, but T-wave is too large in both to be old. Alternative is subacute MI of these vessels.”
“Please send info.”
Case:
This is a 40-something who complained of several 10-20 minute episodes of chest pain over the previous few hours. He had no prior medical history, but is a smoker with a positive family history of CAD. He arrived at 7:30 pain free and had this ECG recorded at 7:32. I will repost it here:
 |
| See above description |
The first troponin was undetectable (cTnT, < 0.01 ng/mL) and he was sent to the observation unit for serial troponins without recording any more ECGs.
Smith comment: this is not acceptable. One should at least perform many serial ECGs to look for either resolution or evolution of these T-waves. Since his pain had resolved and was still gone, one would expect resolution of the large T-waves and minimal ST elevation and this would be diagnostic.
Case continued:
At 8:30 he complained that his pain was returning and another ECG was recorded at 8:42:
 |
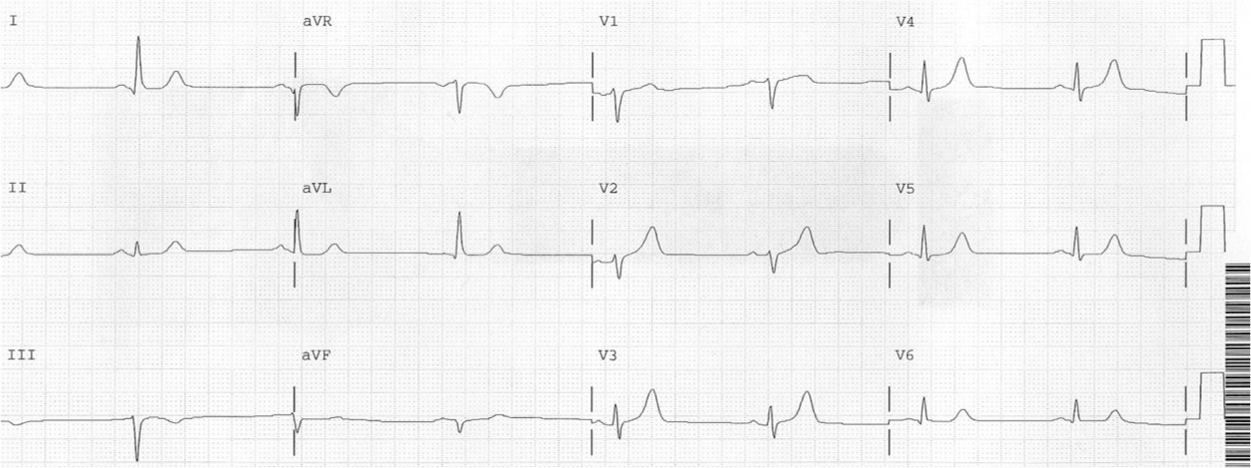
| This is slightly BETTER than the previous There are smaller T-waves, and less STE in aVL, and the reciprocally inverted T-wave in III is not as deep. The down-up T-wave in aVF is now all up. This ECG represents dynamic ACS —Proving that serial ECGs recorded in the ED would have shown resolution of the T-waves.
–Now they are growing larger from what would have been seen on an intervening ECG |
The ECG was interpreted as No Change.
Case continued:
At 8:50 he had “seizure like activity” that resolved (probably an episode of pulseless VT) and was moved to the ICU, where he had this ECG:
 |
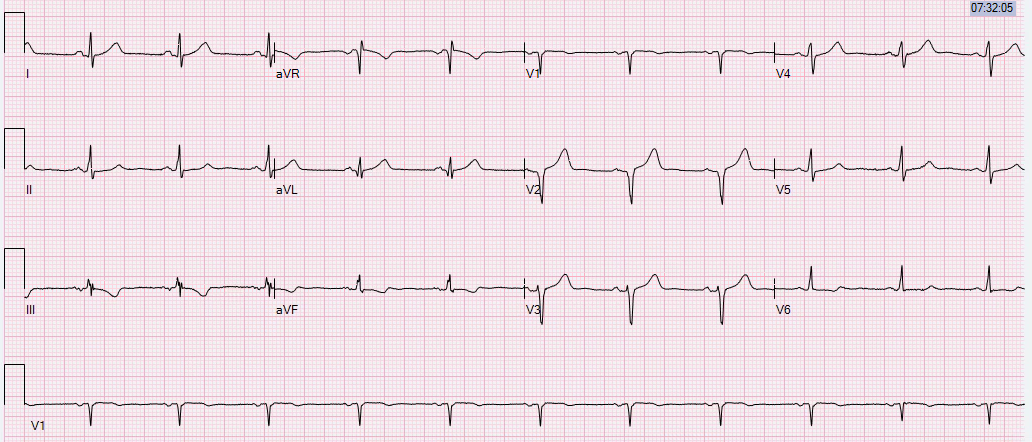
| Obvious proximal LAD occlusion (STEMI) |
Here is his next 12-lead:
 |
| Ventricular Fibrillation is not supposed to be captured on a 12-lead ECG! |
This is after defibrillation and the patient had a pulse and was awake:
 |
| Slow and sick! Take me to the cath lab!! |
This was recorded just before he was taken to the cath lab:

Here is the angiogram:
 |
| Proximal LAD occlusion |
Here annotated with arrows:

Learning Points:
1. Real ECG findings of coronary occlusion can be extremely subtle!
2. Learn to recognize hyperacute T-waves.
3. Learn to recognize down-up T-waves
4. Learn to recognize the reciprocity between aVL and III
5. Troponins are not reliable for diagnosis of early ischemia/occlusion
6. There is still a role for observation!