This was sent by one of our graduates who will remain anonymous.
A 55 year old male with a history of DM and HTN had 2 syncopal episodes, then a third while in the presence of EMS. There was no drug use.
ECG 1. He was put on the monitor and it showed this:
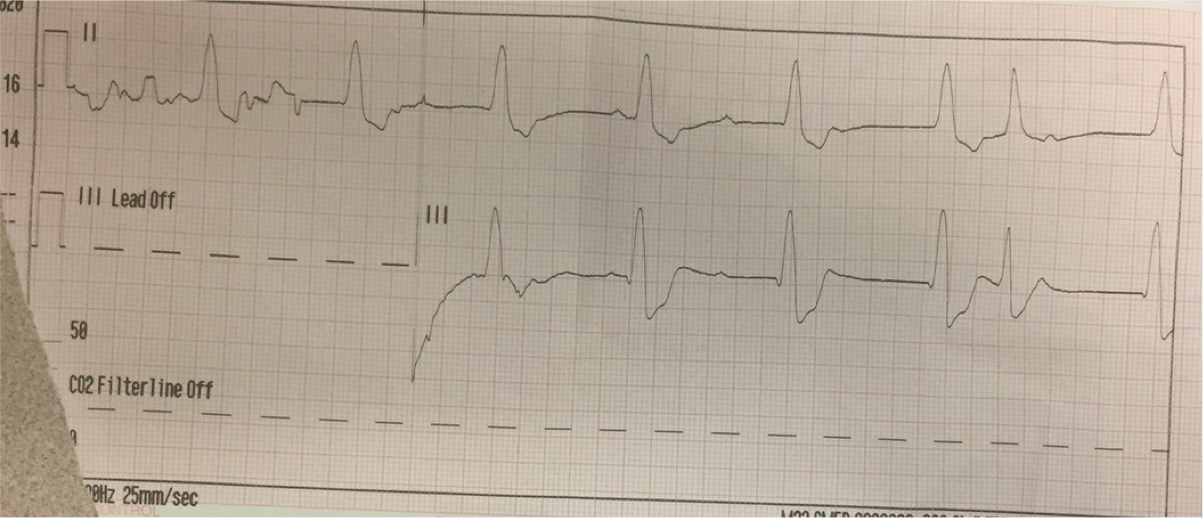 |
| There is a slow, wide complex. There are P-waves that are regular but completely dissociated from the QRS. In fact, they don’t ever conduct. So it is third degree heart block with a ventricular escape. |
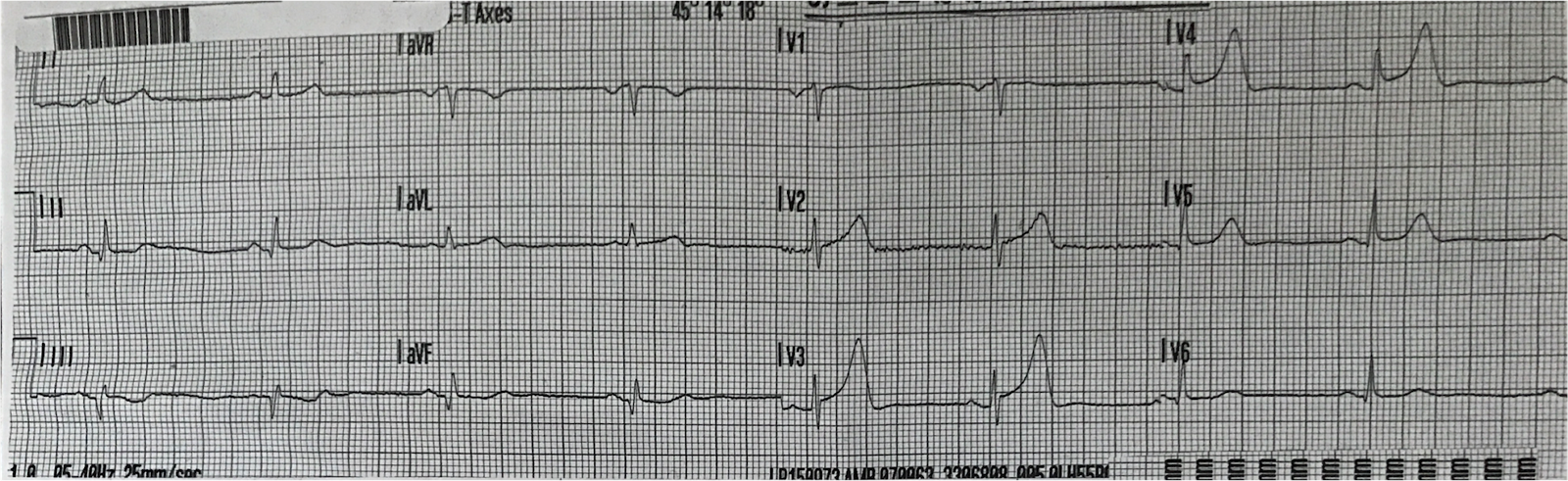
ECG 2. Within minutes, his heart rate normalized:
 |
| Normal sinus rhythm, diffuse non-specific T-wave inversion |
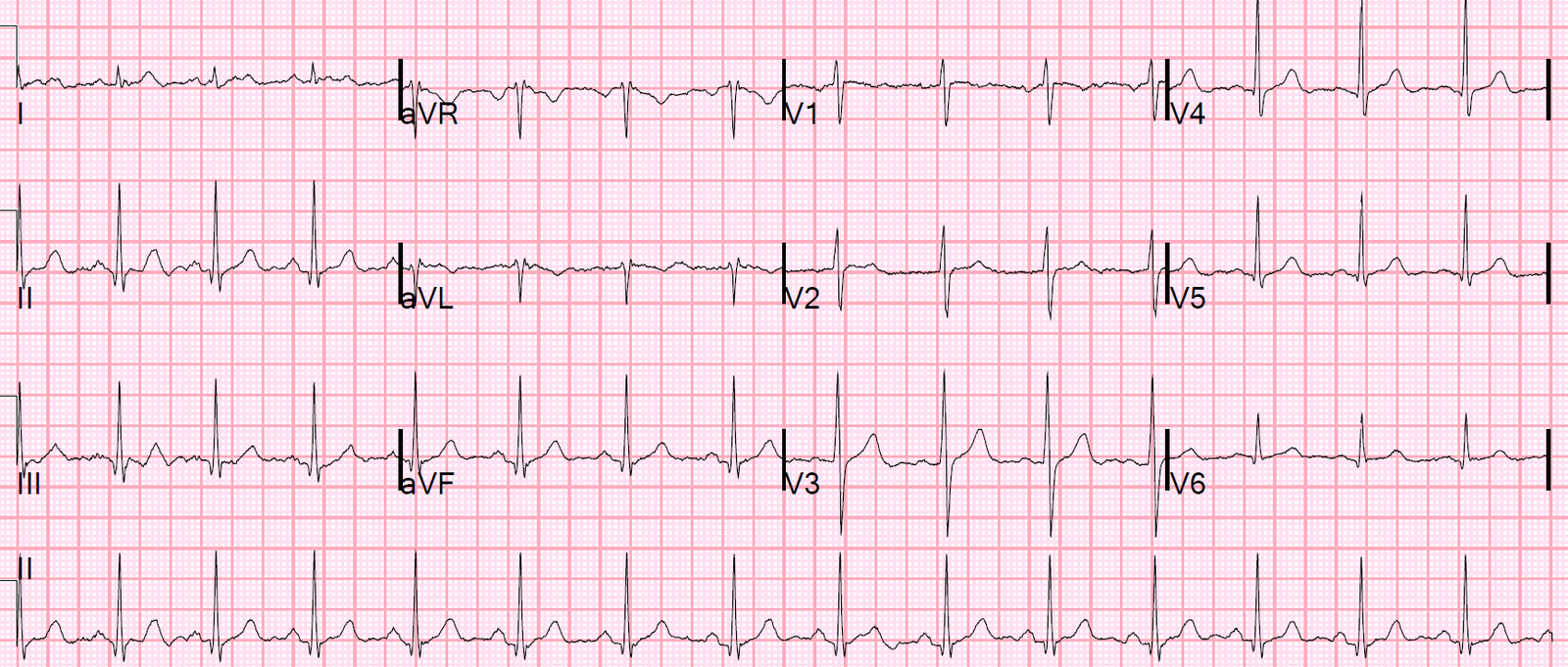
ECG 3. He had no complaints on arrival to the ED. This ECG was recorded at 0209:
 |
| No obvious abnormalities |
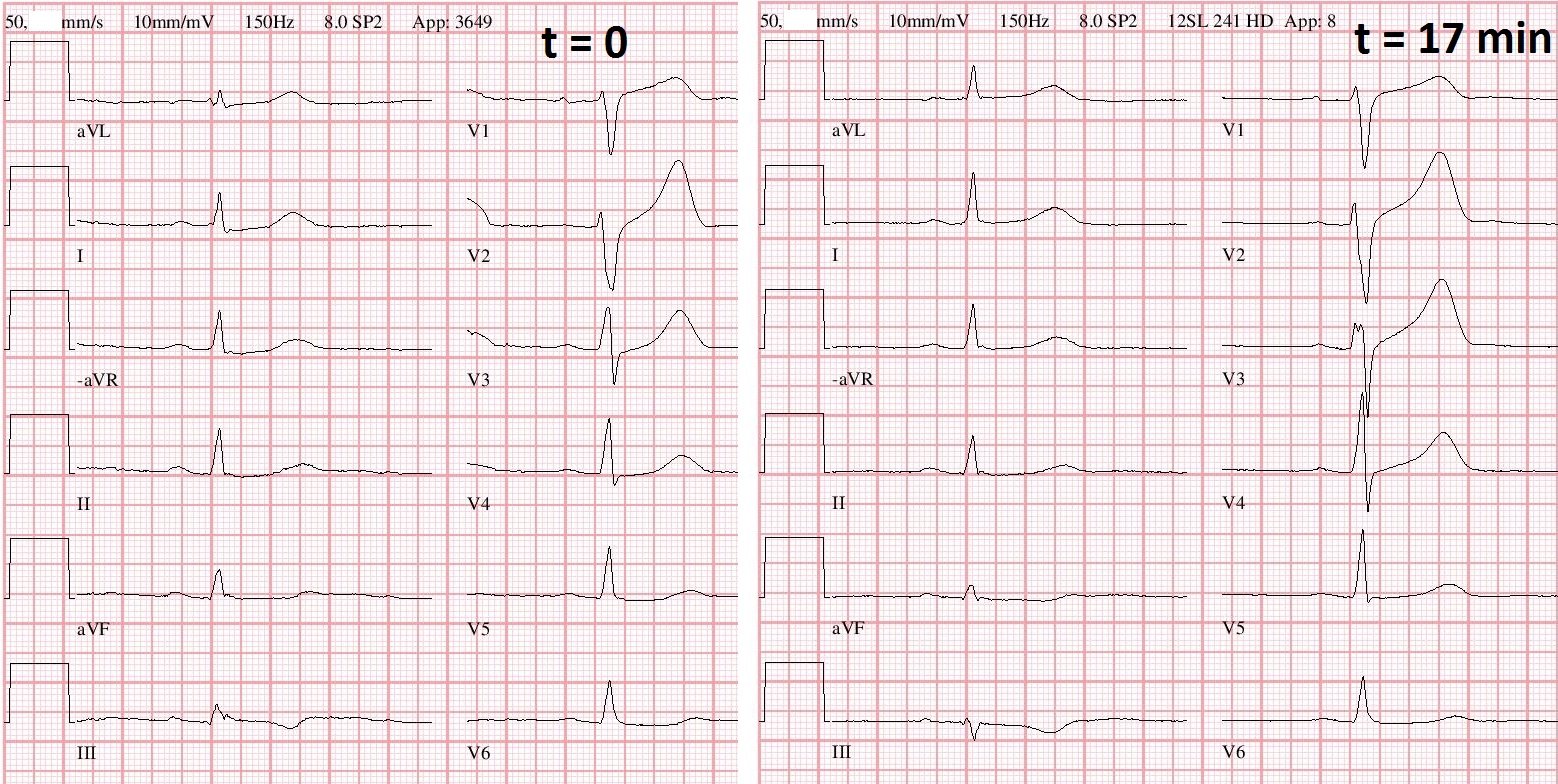
ECG 4. At 0416 (2 hours later) he developed “chest burning.” Here is his ECG:
 |
| Obvious Inferior Posterior STEMI |
ECG 5. His burning quickly resolved, and this ECG was recorded 20 seconds later:
 |
| Resolving ST Elevation (That was fast!!) |
The patient was “rattled” by this experience, felt as if something very bad had just happened.
ECG 6. 7 minutes later, the burning returned. Here was the ECG at 0424:
 |
| This was the doctor’s (my ex-resident’s) response: “He now has ST elevations in a different distribution. Was inferior before, now lateral What the heck? I had been considering coronary vasospasm, but the changing distribution seems to make that less likely.” |
He thought it might be vasospasm of two different coronary arteries.
ECG 7. At 0428 the burning persisted and this was recorded:
 |
| Now they are inferior again!! |
7 minutes later the burning was gone and this ECG was recorded at 0435:
 |
| All STE has resolved again. |
The Cath Lab was activated. Here is the last ECG before he left for the cath lab at 0449:
 |
| There are now inferior reperfusion T-waves (inferior Wellens’ waves!) This supports some degree of infarction. The troponin will be elevated, but not by much as these occlusions were brief. |
Outcome
The cath did not show an occlusion or a definite culprit, but some diffuse non-occlusive disease. No PCI was performed.
I do not have the subsequent troponin.
Subsequent Echo was showed LVH and evidence of hypertrophic cardiomyopathy, without a wall motion abnormality. EF was 65%.
The caregivers (emergency physician and cardiologists) were perplexed about what happened.
What happened?
Why the change in location of ST Elevation??? (There are two explanations below)
Look closely at ECGs 4, 6, and 7:
This was my explanation, which Haim Katalan shows was incorrect (his is below mine)
In 4. and 7., which have inferior ST elevation, the QRS is positive in II, III, and aVF, but negative in aVL (5. also has this QRS axis)
In 6. which has lateral ST elevation, the QRS is negative in lead III, isoelectric in aVF and positive in aVL.
Thus, the limb lead placement was inadvertantly reversed between ECG 5. and 6. And it was inadvertantly reversed back for ECG 7.
So this was a transient inferior STEMI.
Haim Katalan explanation
I
looked carefully at ECG 6-7 and the first ECG with inferior STE. I don’t
think limb leads was misplaced. i) the chest leads looks different in ECG 6 from 7. That can not be accounted for by limb lead swap. ii) Also in
ECG 6 the STE in I & aVL have an action
potential shape completely different from the STD in ECG 7 . iii)
also no P wave axis change as would expected in lead swap.
So my
impression is that it was multi vessel spasm.
Transient STEMI is usually due to brief thrombotic occlusion that then lyses. This occlusion happened several times. The first time it did not result in chest pain but did result in complete heart block. In Acute Coronary Syndrome, a thrombotic event, a culprit is not always found. And the coronary disease may be mild in such cases: the thrombosis just happens at a minimally stenotic, but vulnerable lesion. It is even possible to have thrombosis with a completely normal angiogram, though in less than 1% of cases. In such cases, all the the atherosclerosis is outside the lumen, in the wall of the vessel. So you cannot see it on an angiogram, which is a “lumenogram.” You can see this with intravascular ultrasound, which very well images the thickness of the vessel wall.
Of course vasospasm is usually blamed for these transient ST elevation events, but unseen thrombosis is more common.
The good news is that transient STEMI has a better prognosis than non-transient STEMI, AND ACS with a non-obstructive angiogram has a better prognosis than those with tight stenoses or large thrombus burden.
Learning Points:
1. Always check lead placement when things do not seem right!
2. Beware of Transient STEMI
3. Beware that ACS may have minimal findings on angiogram.