This was sent by a reader who wishes to remain anonymous. Details are at a bare minimum, but it remains instructive.
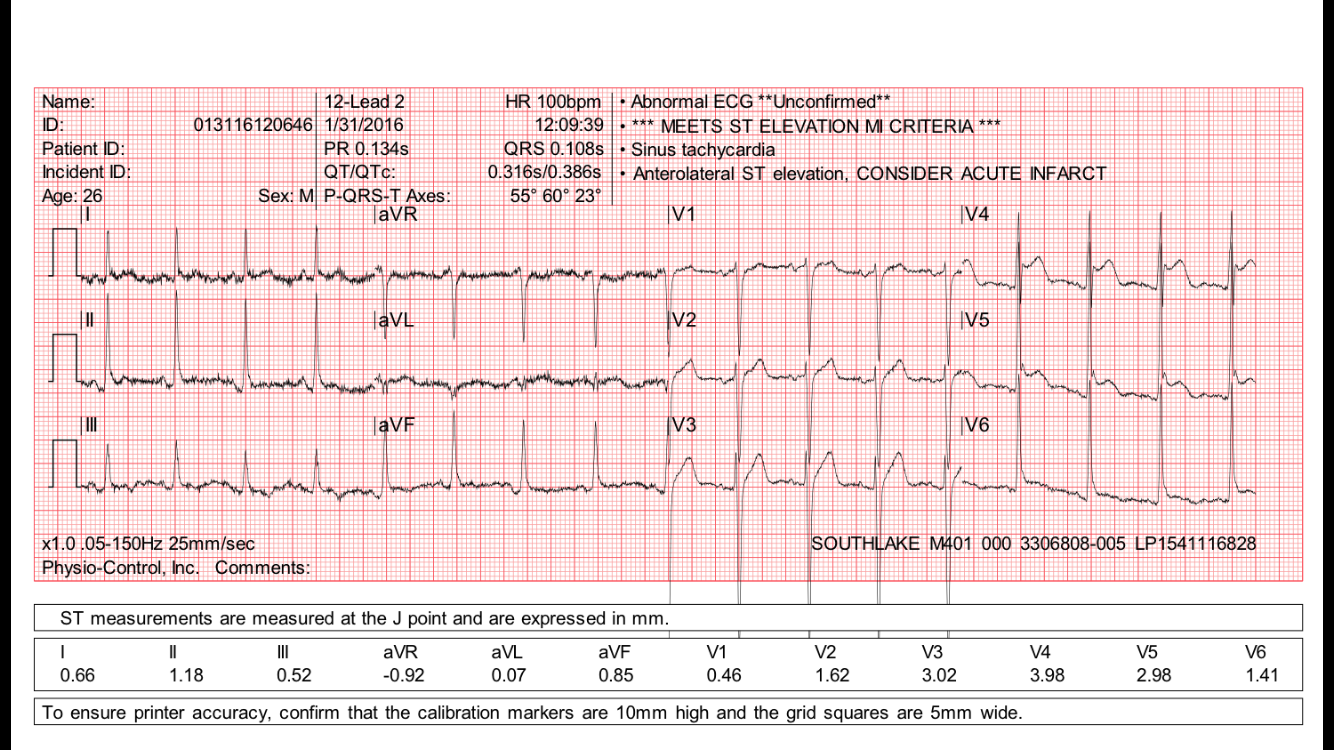
An elderly patient had a good reason for demand ischemia and there was no suspicion of ACS. This ECG was recorded:
 |
|
|
There is sinus tachycardia. Complexes 3, 6, 12, & 15 appear to have some pre-excitation, with secondary repolarization changes.
|
Clinical Course
The pathology leading to the ischemia was treated and resolved. Later, what may have been simply a routine ECG was recorded. If the patient had symptoms at the time of this 2nd ECG, they were not documented. It also is unclear if anyone involved with the patient saw the ECG at the time it was recorded — no clinician commented on it in the chart.
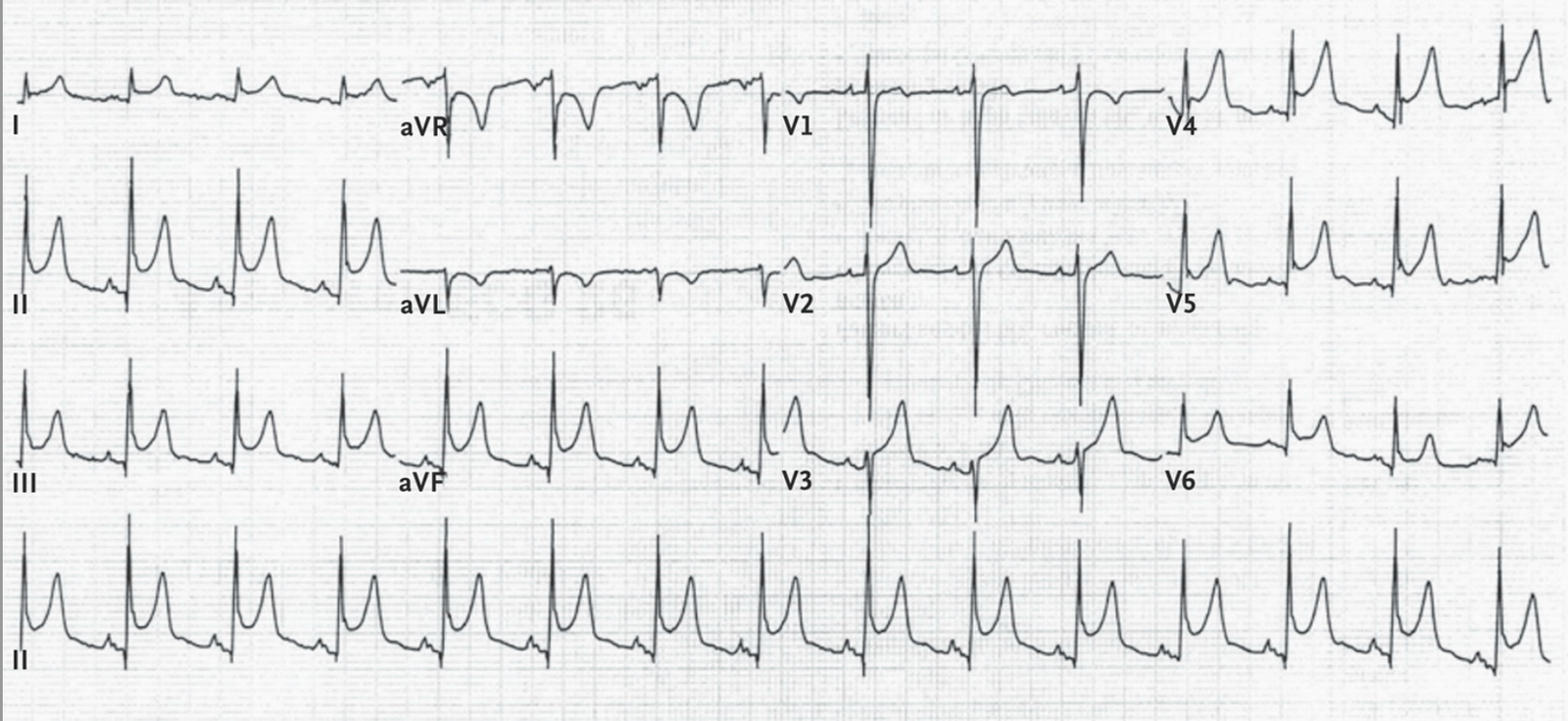
Here it is:
 |
| The cardiologist who read the ECG on the system (who probably did not know the patient or the reason for the recording) read this as “Diffuse Nonspecific ST Elevation, consider Pericarditis” What do you think? |
There is subtle ST elevation in inferior and lateral leads, and subtle reciprocal ST depression in lead aVL and also subtle ST depression in lead V2. This is highly suspicious for acute STEMI, and even meets STEMI criteria in leads V4-V6. It is very unlikely to be pericarditis.
Outcome
Not long after the ECG was recorded, the patient arrested. She was unable to be resuscitated. The autopsy showed an acute RCA thrombosis with 90% occlusion.
Learning Points:
1. You diagnose pericarditis at your (or your patient’s) peril
2. Pericarditis does not have reciprocal ST depression, not in either lead aVL or in V2. This ECG is very specific for STEMI.
3. Even when patients are asymptomatic, or apparently so, they can have life threatening MI. If the ECG has specific signs of MI, as this one does, then do not be fooled by the absence of symptoms.
4. It is very easy to overlook ECG findings if you are interpreting a routine ECG, without knowledge of the patient’s condition (this includes over-reading of ECGs from a list, as was done in this case).