A 63 year old male presented with crushing chest pain. Prehospital BP was 70, but higher in the ED.
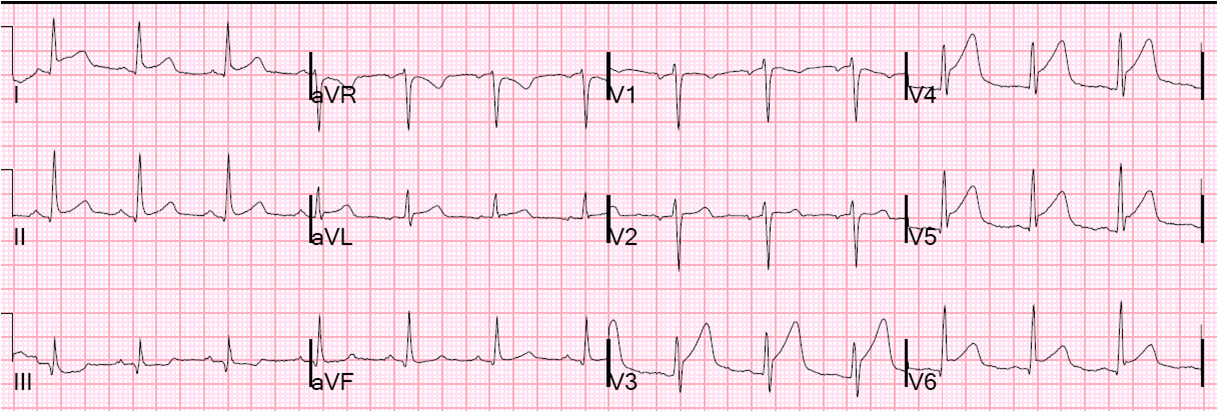
Here is the initial ECG at 1033 PM:
 |
| There is ST segment elevation in V1 – V3. Is it normal ST elevation? There are several reasons why it is NOT normal STE and is due to LAD occlusion. 1) there is ST segment depression in inferior leads, and STE in aVL 2) there is ST depression in V5 and V6. These two features alone make it diagnostic. But one can also use the formula: 3) The QTc is 448, and thus the formula for differentiating normal anterior STE from anterior STEMI has a value of 24.41. (See the side bar of the front page of this blog for the formula). |
Although the ECG is subtle and many or most physicians will not recognize it, it is diagnostic of anterior STEMI. Nothing else has this morphology.
It is important to know that 40-50% of anterior STEMI have upward concavity of the ST segments on the initial ECG.(1, 2, 3)
1. Kosuge M. Am Ht J 1999; 137:522-7. 2. Smith SW. J Em Med 2006;31:69-77 3. Smith SW. Annals of EM 2012;60:45-56
The emergency physician knew that the patient was ill, but did not initially diagnose STEMI. He then noticed the STE in aVL, but not the anterior injury. He did not activate the cath lab immediately, but did immediately consult both an interventionalist and a general cardiologist. They did not see the STEMI, but agreed that this sounded serious and the cath lab was activated.
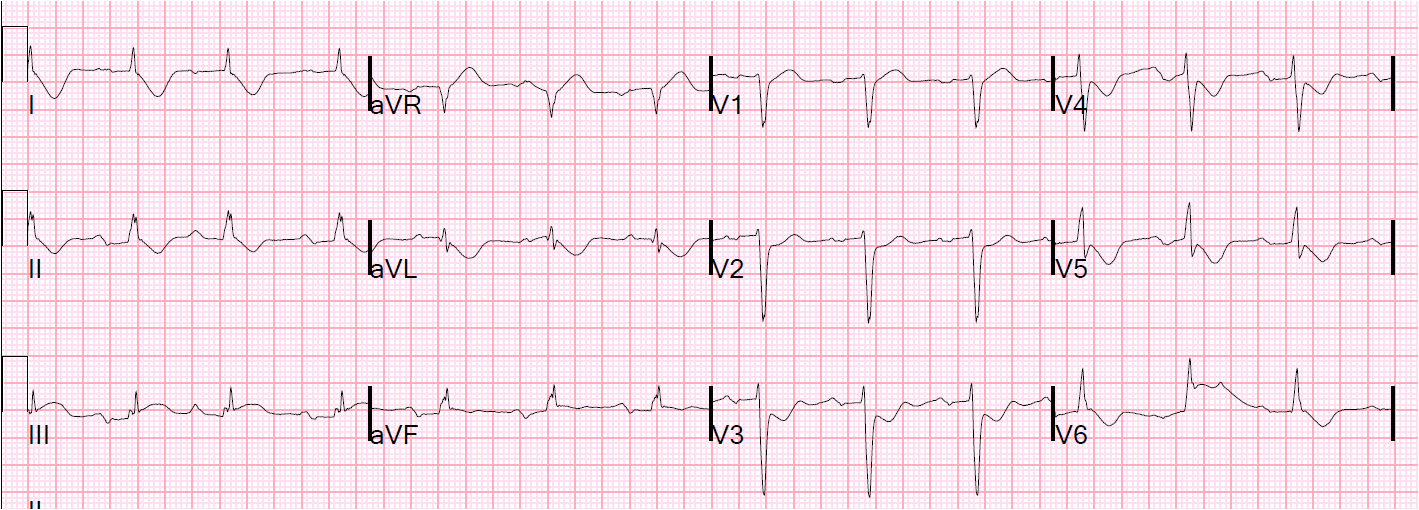
While waiting for the cath lab, this was recorded at 2303:
 |
|
|
At cath, there was severe 3 vessel disease, with an ostial LAD occlusion that was opened. The patient underwent a balloon pump for cardiogenic shock.
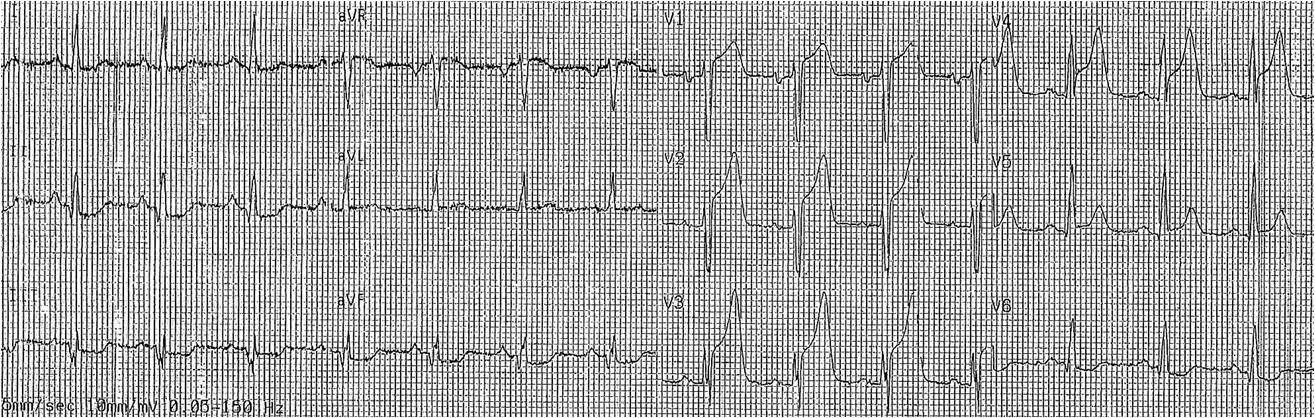
Here is an EKG shortly after leaving the cath lab:
 |
| This appears to me to be sinus rhythm with alternating LBBB and RBBB (not multiform PVCs). There is persistent ST elevation, consistent with poor microvascular reperfusion. The ST/S ratio in the LBBB complexes in V1-V3 is proportionally excessive (>0.25). There is concordant ST elevation in lead V4. There is nearly excessive proportionally discordant ST depression (0.28) in V5 and V6. As for the RBBB complexes |
He went for CABG x 4.