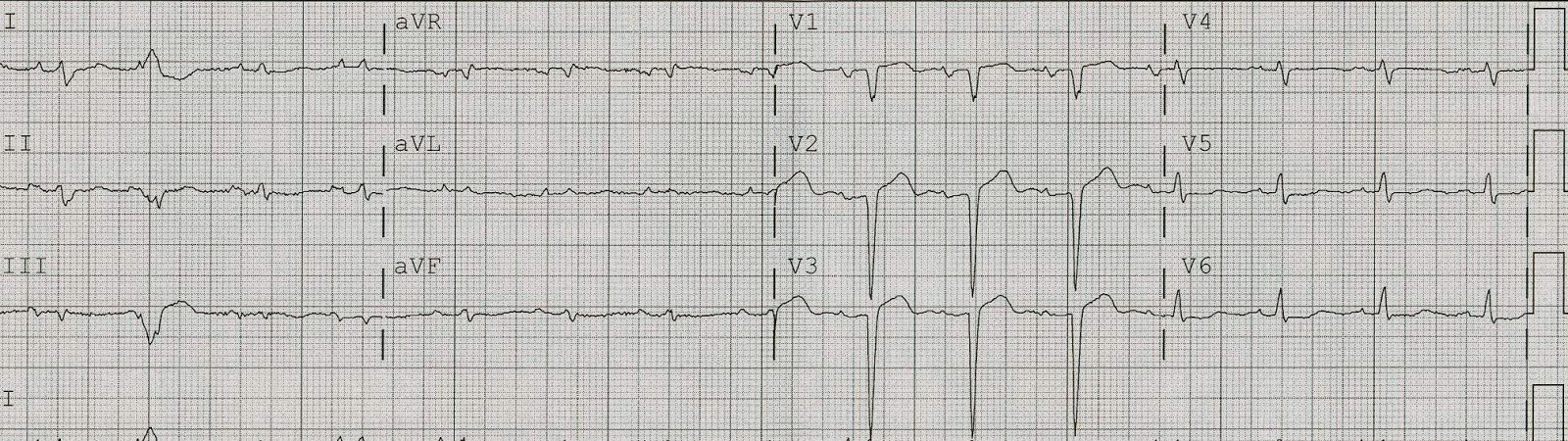
This 41 yo male was cleaning using a chemical and experienced sudden substernal chest burning radiating to both arms with SOB, relieved by sublingual NTG. He called 911 immediately. Here is the prehospital ECG at 1143:
 |
| There are precordial hyperacute T-waves. The QTc is only 392, but there is very poor R-wave progression and the ST elevation, though less than 1 mm at the J-point, is 3 mm at 60 ms after the J-point, which indicates a steep ST segment. The equation value (see side bar of blog, with excel spreadsheet) is 25.1. A value greater than 23.4 indicates that this ST elevation is not a normal variant early repol, but anterior STEMI. More importantly, there is ST depression in “inferior” leads and this is reciprocal to extremely subtle STE in aVL and a T-wave that is massive when compared to the QRS. (There is also some subtle STD in V5 and V6, which is another clue to STEMI). The QRS is so small in aVL that the ST elevation can barely register. The computer had nothing to offer. The medics were worried. |
Here is aVL blown up so you can see the relative size of the T-wave and QRS:
 |
| Tiny T-wave in aVL is giant when compared to the QRS. This is a hyperacute T-wave |
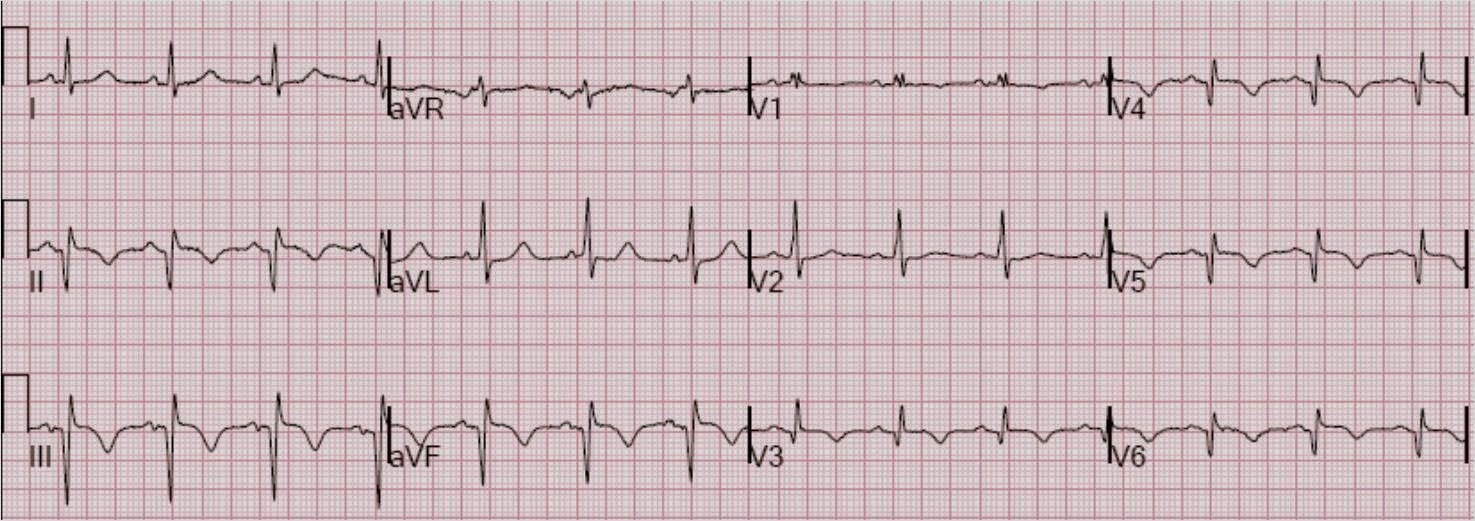
On arrival, the pain was resolved and this ECG was recorded at 1201:
 |
| Notice the R-wave amplitude has recovered. STE at the J-point is no different, but it is less at 60 ms after the J-point because the T-waves are not hyperacute any more. The QTc is 401. The T-waves are less hyperacute. Equation value is now 22.5. There remain some abnormalities in “inferior” leads. |
So we have here a patient with a proximal LAD occlusion that has reperfused on its own (or due to NTG).
The findings of the first ECG, and their difference from the 2nd ECG, were not entirely appreciated, so the cath lab was not activated.
A while later, the first ECG was shown to me without any clinical data and, due to all the characteristics I have described, I was able immediately to say that it is an anterior STEMI. Then, upon looking at the ED ECG, I immediately knew it was reperfused. I knew there was a 90% unstable proximal stenosis with thrombus.
A reperfused anterior STEMI is a dangerous situation. I once had a patient who reperfused the LAD, so I deactivated the cath lab, then he re-occluded and I re-activated the cath lab. The delay caused his death.
This could happen in this case, so it is imperative to at least treat aggressively with antiplatelet and antithrombotic therapy. The cath lab was in use, so this therapy was started, and cardiology was consulted.
Cardiology did an echocardiogram. I was worried that they would find a normal echo. This occlusion was so brief that the anterior wall, though it would have had a motion abnormality during occlusion, could completely and rapidly recover after reperfusion. Thus, a normal echo would give a false sense of security: if normal, it would not rule out previous anterior injury pattern. The ECG does not lie, and in the right hands is better than an echo. This is an unequivocal ECG, especially with the serial findings.
Fortunately, the echo showed some subtle abnormality in the septum, but it was read by one of the world’s experts in echocardiography and perhaps most would not have seen this abnormality and would have dismissed the ECG findings. Then the patient might be admitted and re-occlude (and die?).
The first troponin was normal (so that is of no help).
The two of us talked and arranged for a cath.
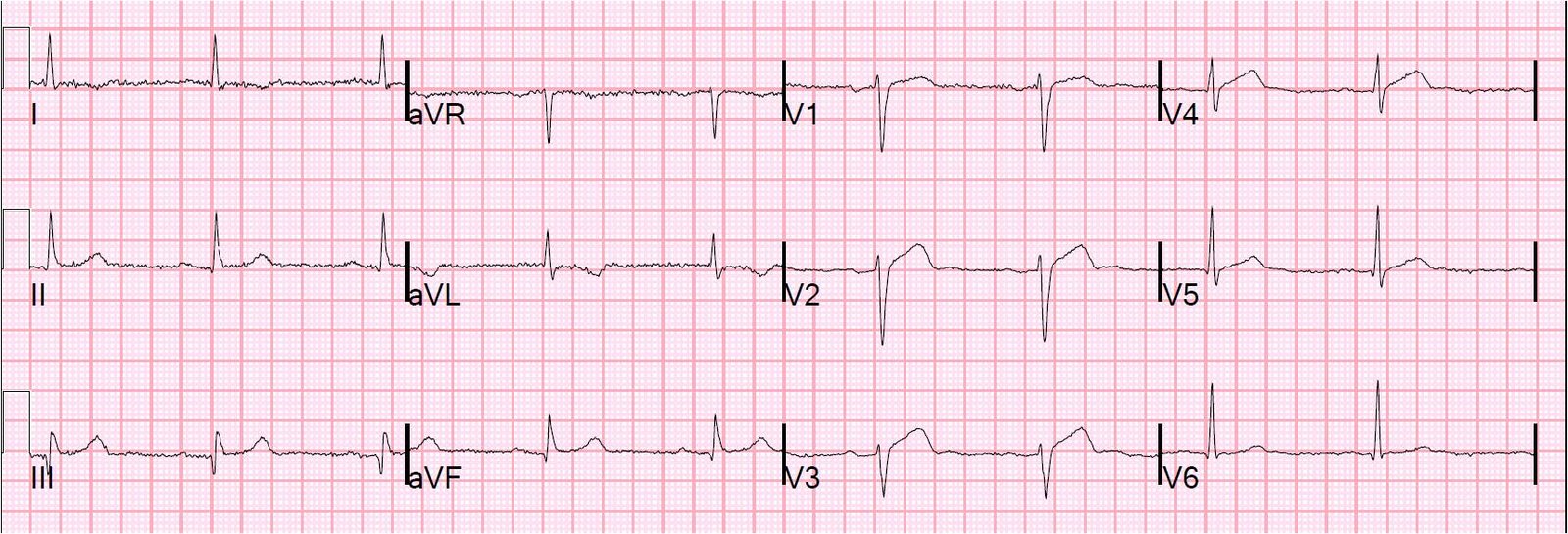
Before his cath, this ECG was recorded at 1321:
 |
| There is further resolution of the findings and it is now normal. |
Cath showed a 95% proximal LAD stenosis with thrombus. A stent was placed.
Here is the ECG the next AM:
 |
| QTc is 378, there is no ST elevation whatsoever. T-waves are much smaller than they were. This probably represents the patient’s baseline ECG, but we can’t know for certain. |
The peak troponin I was 0.9 ng/ml. It is interesting that the ECG did not evolve any T-wave inversion, as might be commonly seen with Wellens’ syndrome. This goes to show that not all brief LAD occlusions result in Wellens’ pattern of reperfusion T-waves.
This was called by the interventionalist and cardiologists a “Non STEMI.” Had the ECG findings not been seen in the ED, no one would ever have known that STEMI was missed.