This was texted to me with the following text:
“Steve any thoughts? I’m interested in your initial reaction and then can give context 😊”
What do you think?
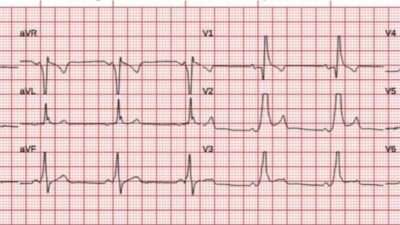
I texted back: “This is a classic ‘fake’ (mimic) of Wellens waves. I think this is a young thin person.”
Why is it not Wellens’?? First, there is very high QRS voltage, including a narrow, large amplitude R-wave in V1 and narrow, large amplitude Q-wave in V6. Hypertrophic Cardiomyopathy is a possibility with high voltage and large R-wave in V1 and narrow deep S-wave in V5-6. There are also what appear to be large U-waves. Mostly, I just recognize this pattern, as I’ve seen it many times in young men. See the link to another example below.
Unfortunately, the Queen of Hearts says “Reperfused OMI with Low confidence.” But she is careful.
Later, I was told that this is a 17 year old with left upper extremity and jaw symptoms after drinking an “energy drink.” They did 60 minute ECG which was identical and all troponins negative. Ultrasound showed no HOCM.
He asked “What do you call this?” And I responded that “It is a variant of Benign T-wave Inversion.”
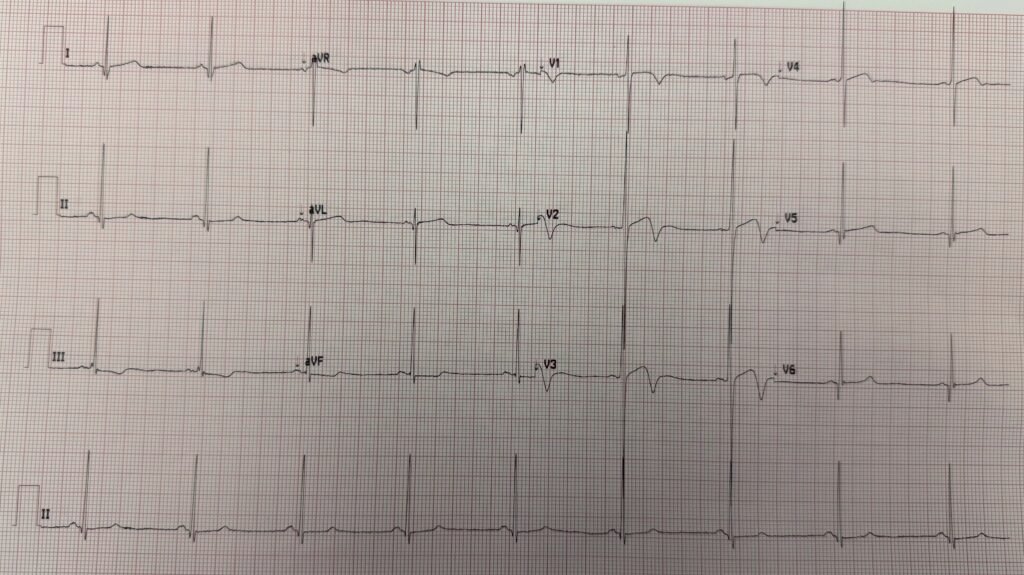
We have had many similar cases; here is one that is nearly identical, with a lot of explanation:
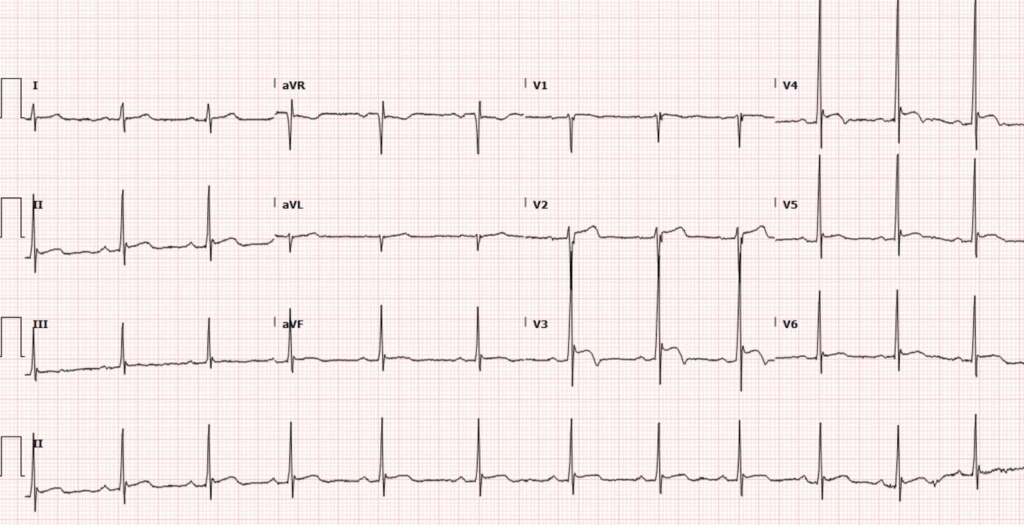
Here are many many cases of the more typical form of Benign T-wave Inversion: Understanding this pathognomonic ECG would have greatly benefitted the patient.
= = =
======================================
MY Comment, by KEN GRAUER, MD (11/25/2025 — updated 11/27/2025):
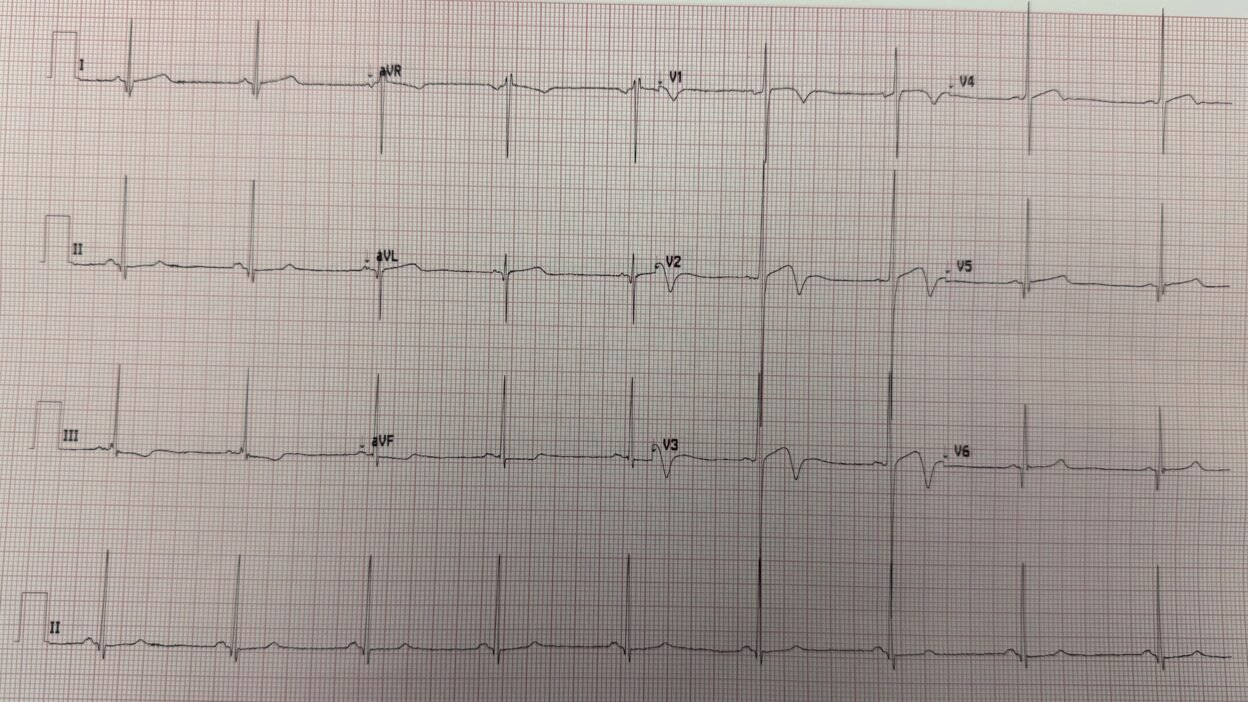
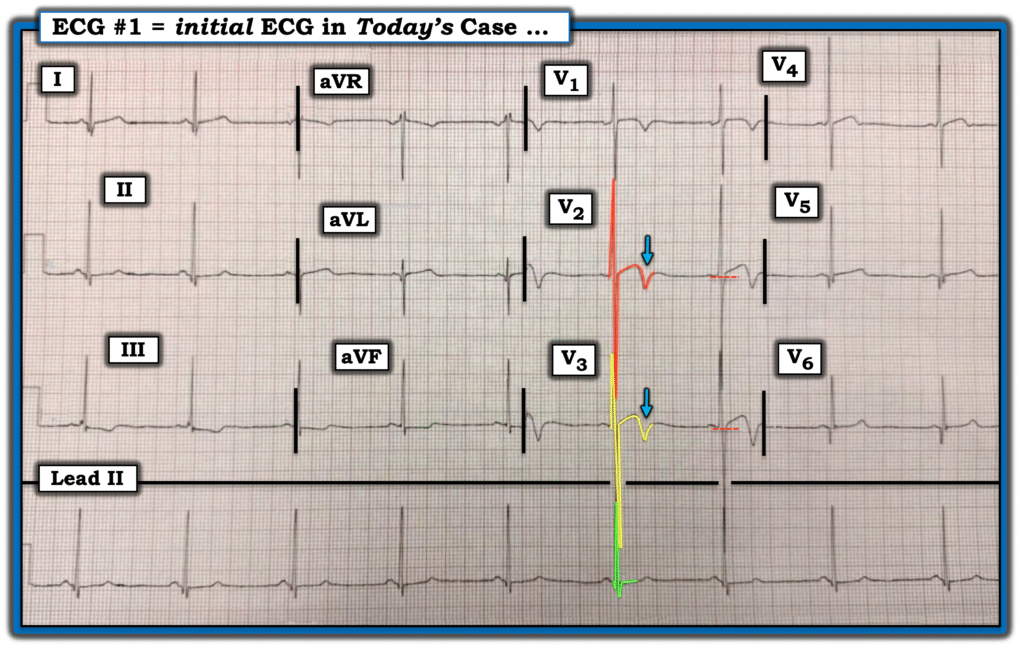
Dr. Smith instantly knew, even without the benefit of any history — that today’s ECG (that I’ve reproduced in Figure-1) — was all-but-certain to represent a “fake”. Why?
- The shape of the ST-T waves in the anterior leads “looks” like a fake (ie, It is marked by a characteristic, slow-rising coving to this slightly elevated ST segment that manifests fairly deep T wave inversion in these same leads that show ST elevation and large R waves).
- QRS amplitude is dramatically increased (Total QRS amplitude of the huge biphasic complexes in V2 and lead V3 exceeds 50 mm in each of these leads! ).
- There is no loss of R wave progression (with a 10 mm R wave in lead V1, that more than doubles this height by lead V2 — whereas with anterior infarction there is loss of R wave forces).
- In view of the bradycardia — the QTc is relatively short.
- Other than anterior leads V1,V2,V3 — the remaining 9 leads in ECG #1 are relatively unremarkable (especially considering the overall marked increase in QRS amplitude).
= = =
Figure-1: The ECG in today’s case — sent to Dr. Smith without clinical info.
= = =
NOTE: We periodically refer to a series of 9 Criteria derived over the years by Drs. Wang and Smith as suggestive of BTWI (Benign T Wave Inversion) — See My Comment in the June 30, 2023 post in Dr. Smith’s ECG Blog.
- Although today’ tracing does not manifest a number of these BTWI criteria — the huge increase in QRS amplitude in the anterior leads, in association with the other morphologic features I describe above results in an ECG “picture” that should immediately suggest to the experienced “eye” that acute OMI is highly unlikely.
- That said — it is wise to be prudent. If a patient with an ECG similar to that shown above in Figure-1 presents to the ED with new chest pain — repreat ECG and at least 2 Troponins (and ideally Echo at the bedside during symptoms to ensure no wall motion abnormality) should be done to definitively rule out an acute event. But in the meantime — Cardiac cath is not needed for this ECG that is all-but-certain to represent a repolarization variant.
===
= = =
NOTE: Although most patients with HCM have an abnormal ECG — the ECG by itself is not at all specific for HCM. Instead, if concerned about the presence of HCM — an Echo is the definitive study!
- For review of the ECG findings expected with HCM (Hypertrophic CardioMyopathy) — Please check out My Comment at the bottom of the page in the June 7, 2025 post of Dr. Smith’s ECG Blog.
= = =
= = =