Because the physician is unlikely to make the diagnosis without the Queen.
This was sent to me by a friend who was working at a small rural hospital without a cath lab.
She wrote this: “The Queen is so helpful. She probably helped me save this guy’s life. As an emergency physician, it is my most coveted tool!”
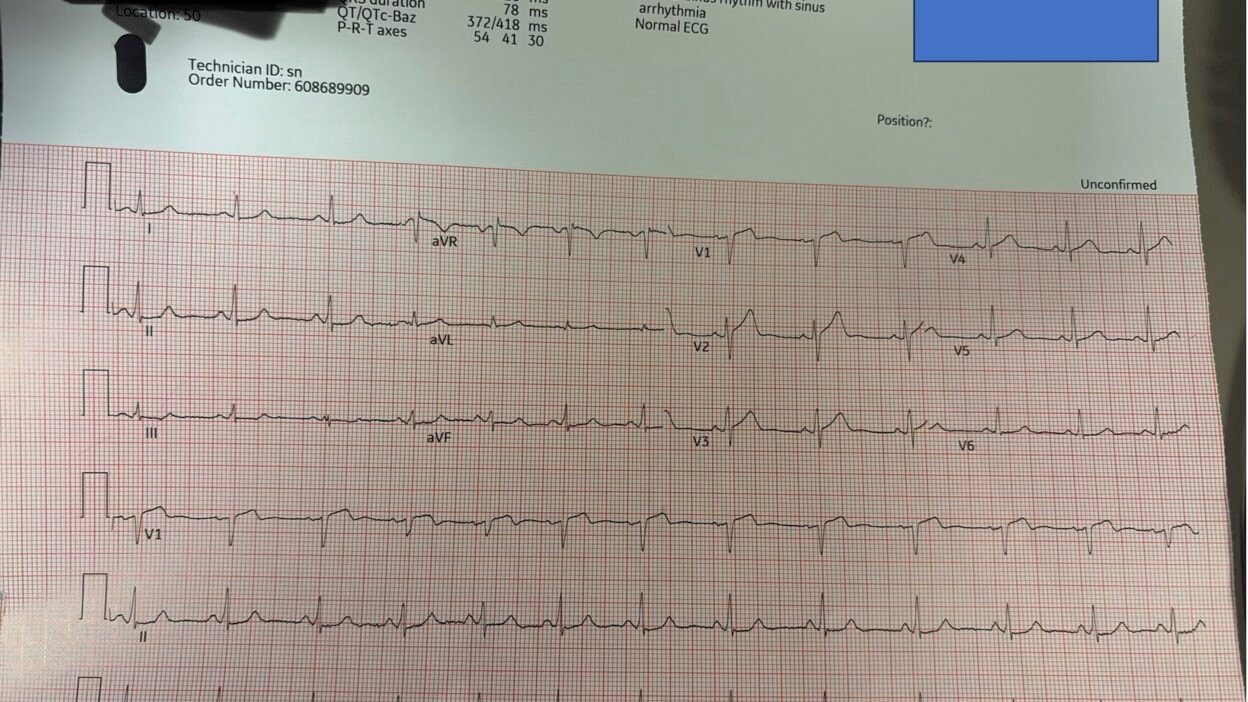
A 60-something male with history of HTN and hyperlipidemia was driving when he had acute onset of chest pain. He arrived in the ED 5 minutes afterwards and had this ECG recorded 3 minutes after arrival:

The conventional algorithm says “Normal ECG”
— What do you think? —
According to the 3 studies below, this ECG should not even be shown to the triage physician because it would be an unnecessary interruption of a busy physician. He/she can wait until full evaluation to see it because there is never an emergency when the algorithm says it is normal.= = =
- Hughes, K.E.; Lewis, S.M.; Katz, L.; Jones, J. Safety of computer interpretation of normal triage electrocardiograms. Acad. Emerg. Med. 2017, 24, 120–124. [Google Scholar] [CrossRef]
- Deutsch, A.; Poroksy, K.; Westafer, L.; Visintainer, P.; Mader, T. Validity of computer-interpreted “normal” and “otherwise normal” ECG in emergency department triage patients. West. J. Emerg. Med. 2024, 25, 3–8. [Google Scholar] [CrossRef]
- Langlois-Carbonneau, V.; Dufresne, F.; Labbé, È.; Hamelin, K.; Berbiche, D.; Gosselin, S. Safety and accuracy of the computer interpretation of normal ECGs at triage. Can. J. Emerg. Med. 2024, 26, 857–864. (accessed on 5 January 2025). [Google Scholar] [CrossRef]
== =
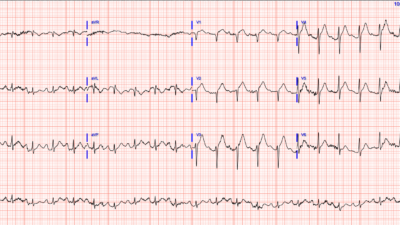
Smith: There is ST Elevation and Hyperacute T-wave in V1-V3. There is a touch of ST depression in V6. There is also minimal STD in inferior leads. So this is Precordial Swirl pattern of LAD occlusion proximal to the septal perforator, indicating septal OMI.
For this ECG which is diagnostic of OMI, the conventional algorithm does not even state that there are “Non-specific ST-T abnormalities”!! Instead, “Normal”!!
We published this study on Precordial Swirl:
Another relevant publication: We showed that, of 42 Cases of OMI that I recognized as OMI on the ECG but the conventional algorithm diagnosed as completely normal, the Queen of Hearts diagnosed 80% as OMI. Artificial Intelligence Detection of Occlusive Myocardial Infarction from Electrocardiograms Interpreted as “Normal” by Conventional Algorithms
I have dozens of cases here of “Normal ECG by Computer Algorithm”. Most are OMI (and diagnostic of OMI). Many are hyperkalemia or long QT.= = =
Case continued:
The physician was uncertain about this ECG, so she put it through the Queen of Hearts and here is the result:

More Queen output:
- STEMI millimeter criteria: Does NOT meet
- Numerical = 0.99 (nearly absolutely certain!)
- Hyperacute Twave score: 0.66 (just below the 98% specific cutoff of 0.70)
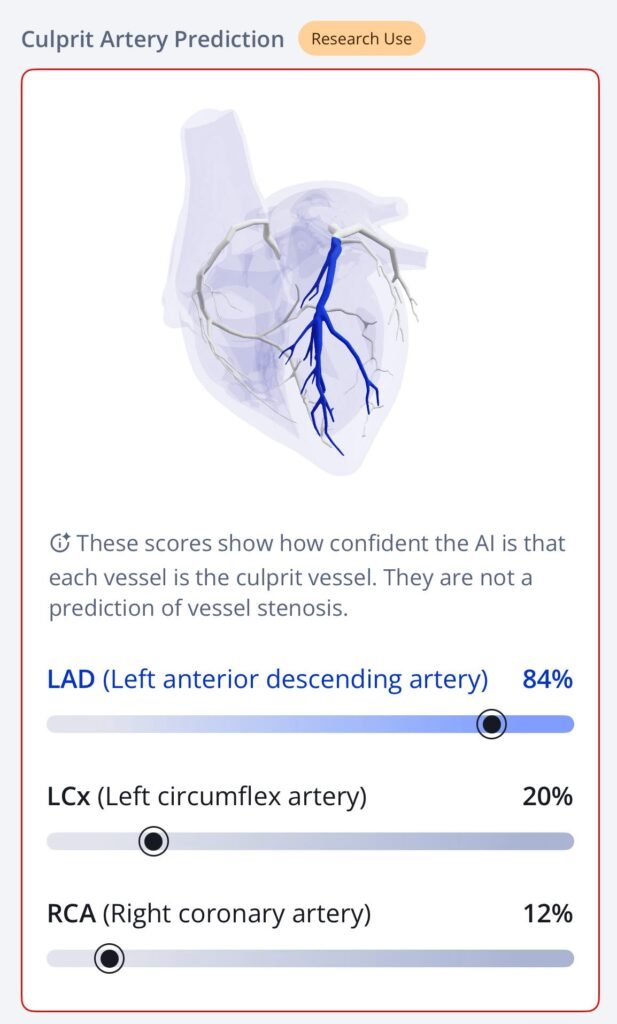
- Artery: Left Anterior Descending 86% probability. See artery visualization below!!
New PMcardio for Individuals App 3.0 now includes the latest Queen of Hearts model and AI explainability (blue heatmaps)! Download now for iOS or Android. https://www.powerfulmedical.com/pmcardio-individuals/ (Drs. Smith and Meyers trained the AI Model and are shareholders in Powerful Medical). As a member of our community, you can use the code DRSMITH20 to get an exclusive 20% off your first year of the annual subscription. Disclaimer: Certain AI ECG Modules are CE-marked medical devices under EU MDR and are certified for marketing only in the European Union and the United Kingdom. PMcardio technology has not yet been cleared by the US Food and Drug Administration (FDA) for clinical use in the USA, and is not yet available in the USA.
Due to the Queen’s result, she activated the cath lab at the referral hospital.
- Just as the patient was leaving, the first troponin returned undetectable.
- The door-in-door-out time was 41 minutes.
On arrival to the PCI hospital, the providers were confused about whether the patient should go to the cath lab because “the ECG was not technical criteria.” But because the referral doctor had activated the pathway, they took the patient.
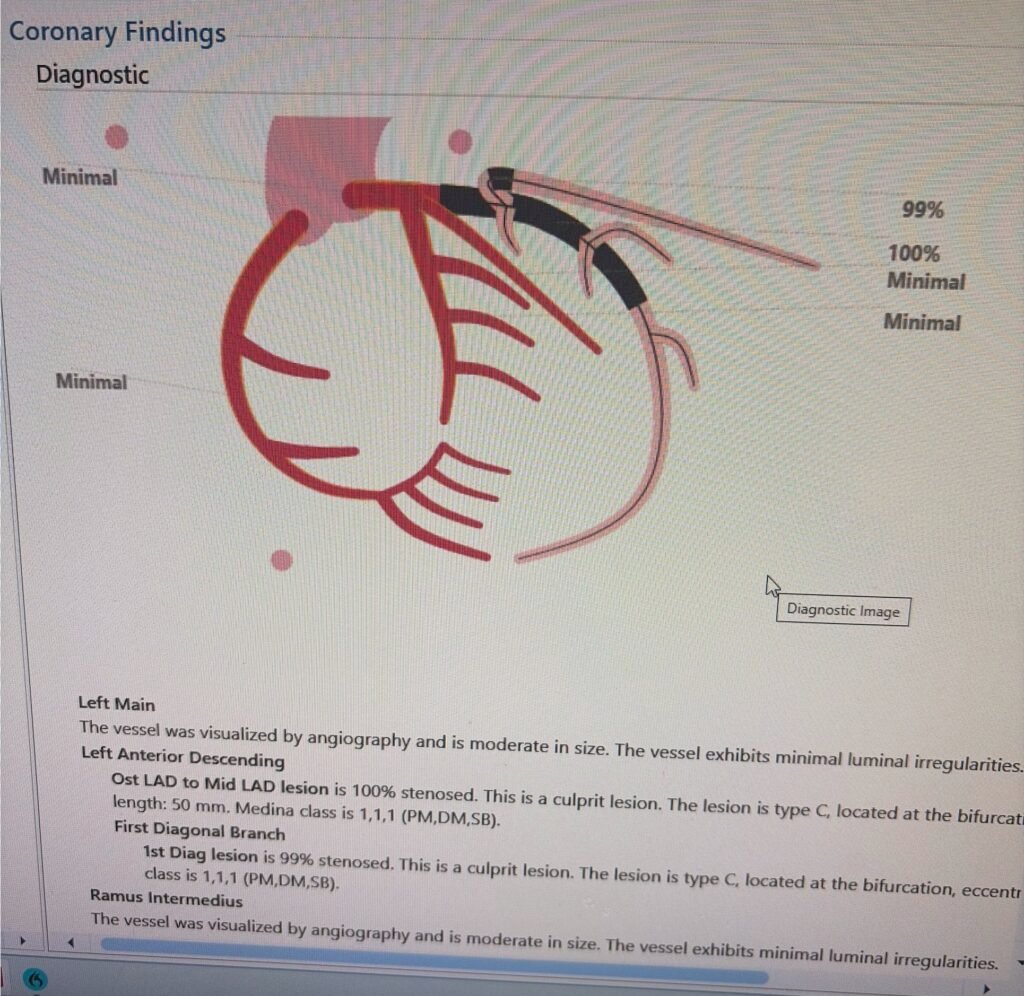
Angiogram
- There was a 100% ostial (very proximal) LAD occlusion. According to the schematic below, the occlusion was proximal to the septal perforator, with Septal OMI just as predicted. Frankly, it does not look like that to me but I am far from expert at angiograms.
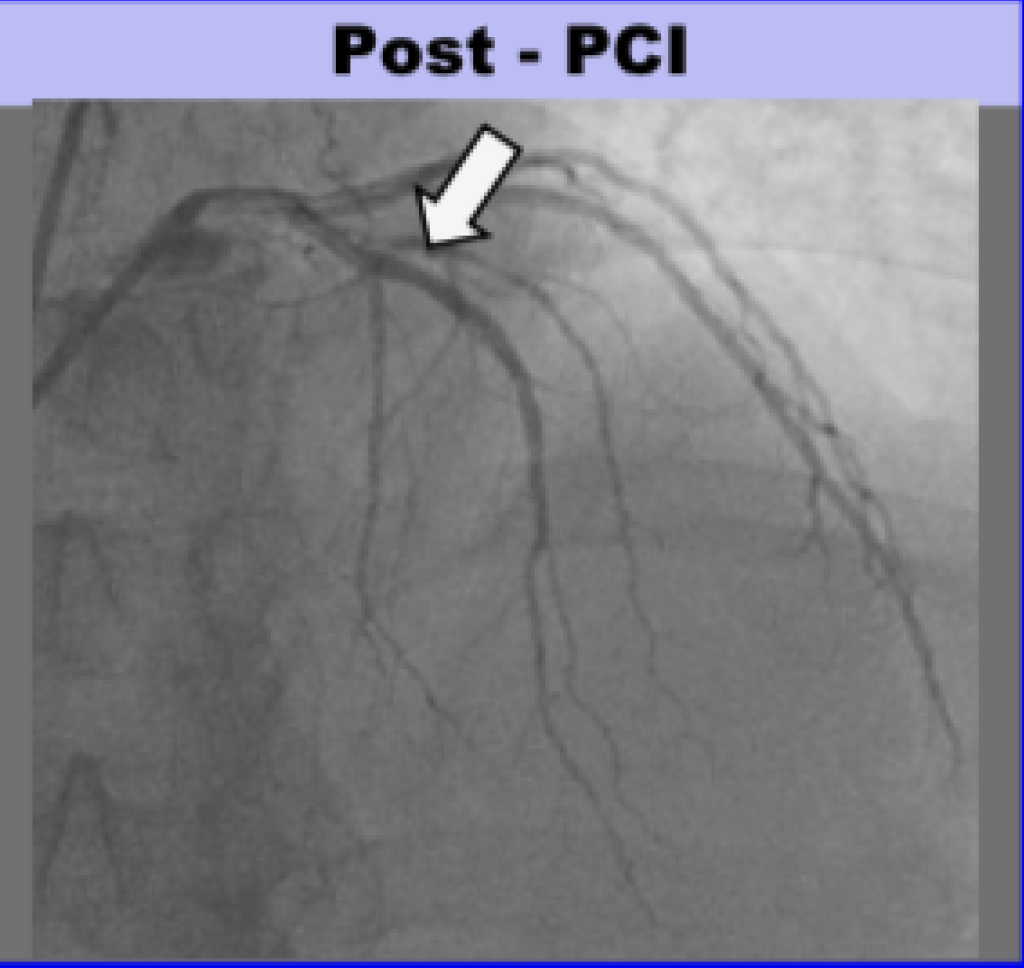
Here is the angio before and after PCI, and a schematic:
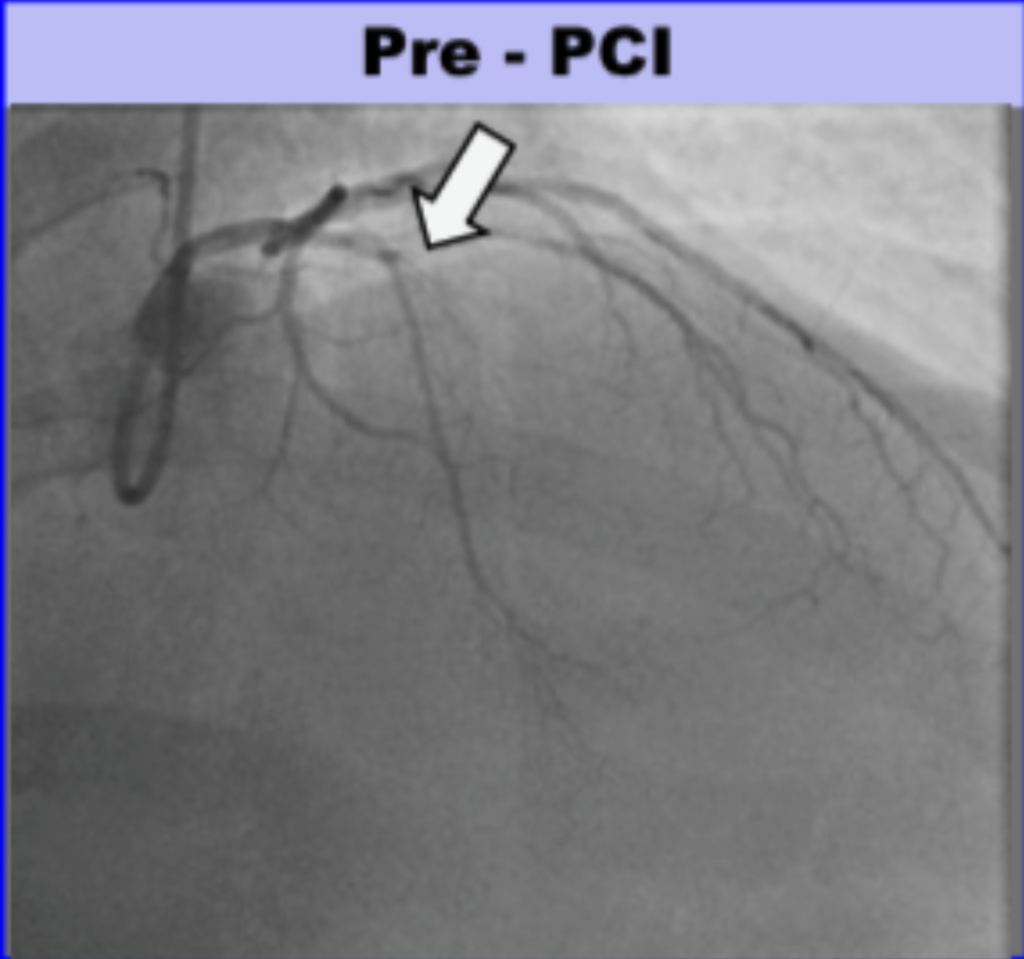
Total time from door at outside hospital to balloon at PCI hospital was 88 minutes! (In transfer cases, guideline acceptable time is 120 minutes from first medical contact to balloon)
- Time from symptom onset to ED = 5 minutes
- ED to ECG = 3 minutes.
- ECG to decision was 5 minutes. This is thanks to the Queen!
- Door-in-door-out was 41 minutes.
- Transport time was 14 minutes.
- Door (PCI center) to balloon time was 33 minutes.
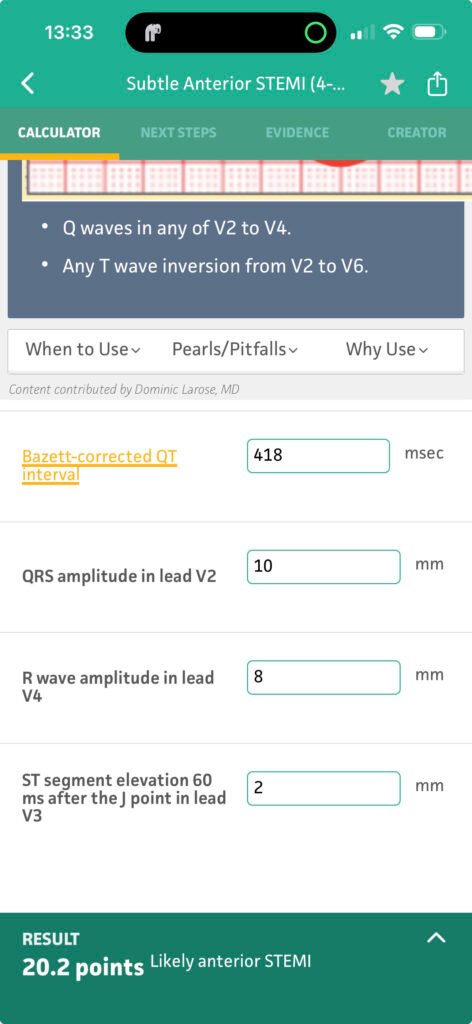
Here the result of the 4-variable formula that differentiates the STE of Normal Variant STE from the STE of LAD Occlusion:
Learning Points:
- Frequently, an ECG which is diagnostic of OMI will be diagnosed as Totally Normal (not even “Nonspecific ST-T abnormalities”) by the conventional algorithm.
- The Queen of Hearts will diagnose OMI 80% of the time when the ECG is diagnostic but the conventional algorithm says “Normal ECG”.
- Precordial Swirl is a proximal LAD OMI Pattern that frequently is missed.
- Frequently, the first troponin in a total coronary occlusion is undetectable.
- You should run all ECGs through the Queen of Hearts to be certain you are not missing a subtle OMI.
= = =
======================================
MY Comment, by KEN GRAUER, MD (4/29/2026):
In 2026 — Conventional ECG algorithms (which literally includes all ECG interpretation algorithms other than QOH) have no place in the diagnostic assessment of patients who present to the ED for acute CP (Chest Pain).
- This concept has been proven time-and-time again in numerous posts on Dr. Smith’s ECG Blog. Reasons for this truism are simple:
- i) Conventional ECG algorithms focus on identifying STEMIs — but insisting on millimeter-based STEMI criteria will miss up to 1/3 of acute OMIs in which there is acute coronary occlusion (and even in those OMIs that are picked up — waiting until STEMI criteria are eventually satisfied often delays the time until reperfusion occurs by too many hours!).
- ii) Conventional ECG algorithms have poor sensitivity for picking subtle abnormalities (Witness the erroneous computerized interpretation of “Normal ECG” in today’s case — in which ECG findings are not even that subtle).
- iii) Conventional ECG algorithms fail to take into account the history (Witness today’s case of a 60-something man with risk factors, who develops acute CP severe enough to immediately seek emergency care — thereby within minutes (!) placing this patient in a higher-risk group for having an acute event well before we get to look at his initial ECG!). Our threshold for accepting even subtle abnormalities as suspicious for OMI needs to be lowered when assessing “higher risk” patients who present with a worrisome history of acute CP!
Bottom Line: Emergency physicians need to be interrupted to review the ECG of any and all patients who present to the ED for acute CP:
- With training and experience in the OMI Paradigm — it should not take long for emergency physicians to review the initial ECG for signs of acute coronary occlusion (ie, less than a minute).
- Decision-making is easy when STEMI criteria are clearly met ( ==> the need for prompt cath with PCI is quickly established).
- For the many acute CP patients in whom STEMI criteria are not clearly satisfied on the initial ECG (as in today’s case) — Ready access to the QOH algorithm optimizes accuracy — and expedites the process (assuming of course, that the QOH interpretation is readily accessible at the time the ED physician is reviewing the tracing). In this way — the QOH interpretation serves as a check that may both educate as well as obligate the ED physician to reexamine the case if by chance QOH suspects an OMI that was not appreciated (as so effectively occurred in today’s case).
- Additional Benefits to accrue from “interrupting” the busy ED physician to take a quick look at any and all ECGs from acute CP patients include the following:
- If the initial ECG is equivocal (ie, non-diagnostic) — the ED physician can give the order to repeat the ECG within 10-20 minutes (thereby not allowing hours to pass — as so often occurs when no one is made aware of the case or the initial ECG). Surprisingly often within a short period of time — acutely evolving OMIs will manifest “dynamic“ ST-T wave changes that confirm the the need for prompt cath.
- Learning occurs! For example, in today’s case — Providers at the PCI hospital were confused about whether the patient should go to cath. Fortunately, they honored HM’s decision to activate the cath lab — and these providers clearly learned from the proximal LAD occlusion on cath that today’s initial ECG did in fact represent an acute OMI that they hopefully will recognize more easily the next time (especially if they have ready access to QOH for assistance!).
= = =
A Closer LOOK at today’s initial ECG
I find the best way to optimize use of the QOH interpretation — is for me to first formulate my unbiased opinion — that I can then compare to the QOH interpretation.
- In today’s Case — I knew within seconds that the initial ECG in this patient with acute CP represented an acute OMI until proven otherwise.
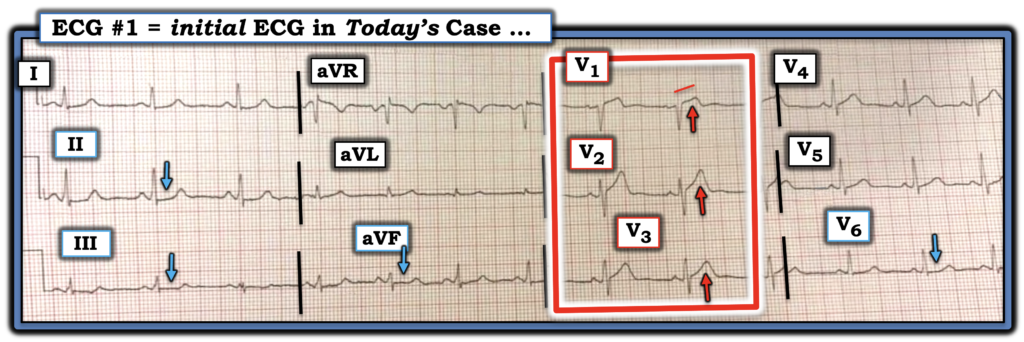
For clarity in Figure-1 — I’ve labeled KEY findings in today’s initial ECG.
- My “eye” was immediately captured by the ST-T wave appearance in leads V1,V2,V3 (within the RED rectangle) because: i) The ST segment straightening with subtle-but-real ST elevation in lead V1 is clearly abnormal (disproportionate) to the small S wave amplitude in this lead (Lead V1 simply should not normally show ST segment straightening and elevation in an acute CP patient); — and, ii) Neighboring leads V2,V3 continue the hyperacute appearance, in that their ST-T waves are “fatter”-at-their-peak and wider-at-their-base than they should be (ie, disproportionate) given how small the S waves remain in these leads.
- And — We know that the ST-T wave findings within the RED rectangle are “real” — because of the subtle-but-clearly-abnormal ST-T wave flattening (with subtle ST depression) in each of the inferior leads (BLUE arrows in these leads). In the context of acute CP — this finding of reciprocal inferior lead changes strongly supports the likelihood of acute proximal LAD occlusion.
- Total time for me to appreciate these findings = less than 5 seconds.
- P.S.: Awareness of the Precordial “Swirl“ pattern that Dr. Smith references in his discussion allows us to note the flattened ST depression in lead V6 (BLUE arrow) — but to emphasize that appreciation of this subtle lead V6 finding is not essential to immediately know from this initial ECG that prompt cath is needed.
= = =
Figure-1: I’ve labeled the initial ECG in today’s case.
= = =
Conclusions:
The unfortunate clinical reality (proven too-numerous-to-count times in the cases we regularly present in Dr. Smith’s ECG Blog) — is that most clinicians (including cardiologists) are simply not able to reliably identify subtle signs of acute OMI.
- The principal reason for this inability is persistent dependence on the outdated STEMI paradigm that misses and/or substantially delays recognition of too many acute coronary occlusions that could (and should) be picked up by application of OMI Paradigm principles.
Appreciation of Dr. Smith’s Learning Points facilitates the process — and merits repetition.
- Conventional ECG algorithms should not be used. They are inaccurate and misleading for assessing the patient with acute CP.
- Recruitment of the QOH (Queen-Of-Hearts) AI application to assist emergency providers facilitates and expedites recognition of acute OMIs with highly impressive accuracy — with extra benefit of showing (teaching) emergency providers how quickly they can identify the important subtle findings of acute coronary occlusion.
- Assistance from QOH is especially important given the documented caveat that the 1st Troponin value may be normal (especially in cases like today’s patient — in which the patient presented to the ED so soon after the onset of symptoms!).
= = =
= = =