This was sent by an “avid reader.” The case was from his hospital, which does not have a cath lab.
Case
A 60-something male was sent in from a cardiologists’ office after presenting there with chest pain. The office ECG is unavailable.
The pain had been intermittent for a few days, but worse on the day of admission.
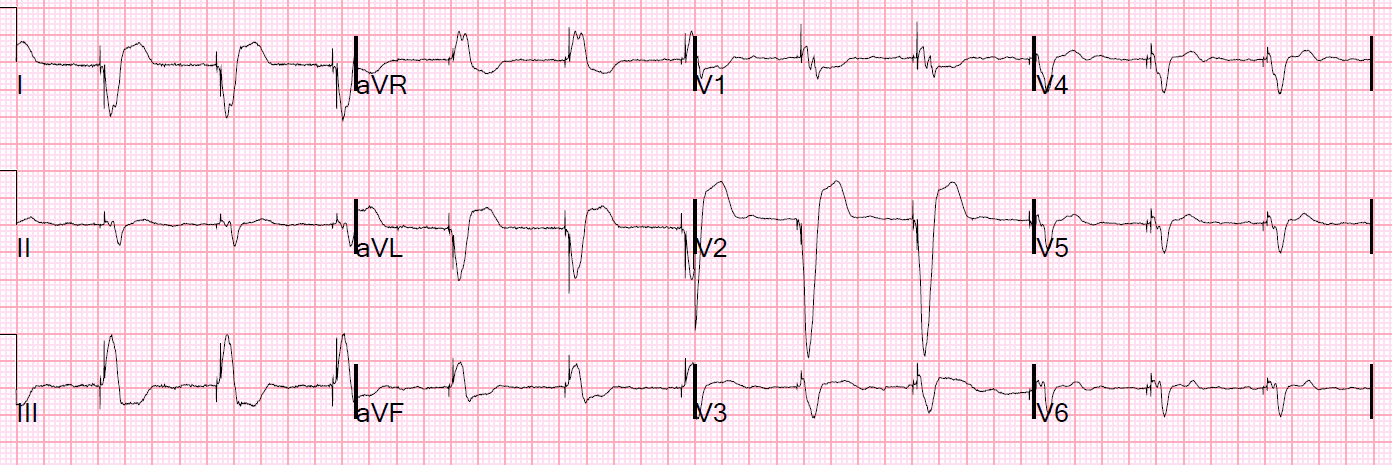
Here was the initial ECG:
 |
| To me, and to him, this is an obvious acute LAD occlusion. There are hyperacute T-waves, especially in V2, plus other more subtle findings. If you use the 4-variable formula:STE60V3 = 2.5 QTc = 398 RAV4 = 3 QRSV2 = 15 Value = 20.28, confirming LAD occlusion (18.2 is the most accurate cutoff). |
The Emergency physician and the cardiologist concluded: “No STEMI. Admit here. Do not transfer.”
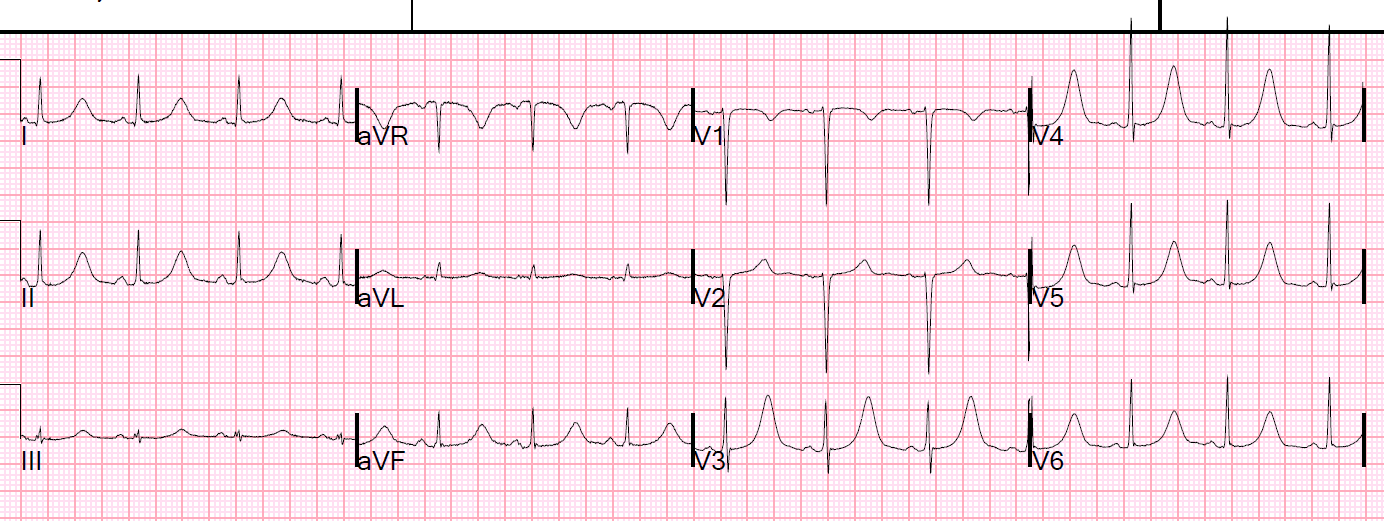
At a minimum, this patient needs ECGs recorded every 15 minutes. This was not done. The next ECG was recorded 90 minutes later:
 |
| Now it is an obvious anterior STEMI. The ST Elevation even meets “criteria” now. Why does the computer not diagnose it? |
The first troponin I returned at 1.5 ng/mL. A repeat returned at 2.5 ng/mL. Still no 3rd ECG recorded.
At this point, the patient developed cardiogenic shock, and another ECG, at 270 minutes (3 hours after the 2nd ECG), was recorded:
 |
| Now there is massive ST elevation. There are multiple PVCs. There is clear STE in aVL, with inferior reciprocal ST depression. |
The patient was transferred by helicopter to a PCI facility.
Cath: “Entire left system occluded.” (including left main). Ejection fraction 10%. Too ill for CABG surgery.
I do not have further outcome, but his chances of survival are not good.
Learning point:
Do not wait for STEMI if you find an OMI.
We all have much to learn. Hopefully this physician will learn from this one, so that future similar patients will not be similarly doomed.
![]()
===================================
Comment by KEN GRAUER, MD (5/7/2019):
===================================
This tragic case is one to learn from. Unfortunately, those in need of the most learning ( = those close-minded colleagues of the “avid reader” who sent in this case) are the least likely to profit from mistakes made. Dr. Smith has already emphasized many KEY points about this case.
- I’d add the following thoughts regarding the initial ECG obtained on this 60-something man with new-onset chest pain (Figure-1):
 |
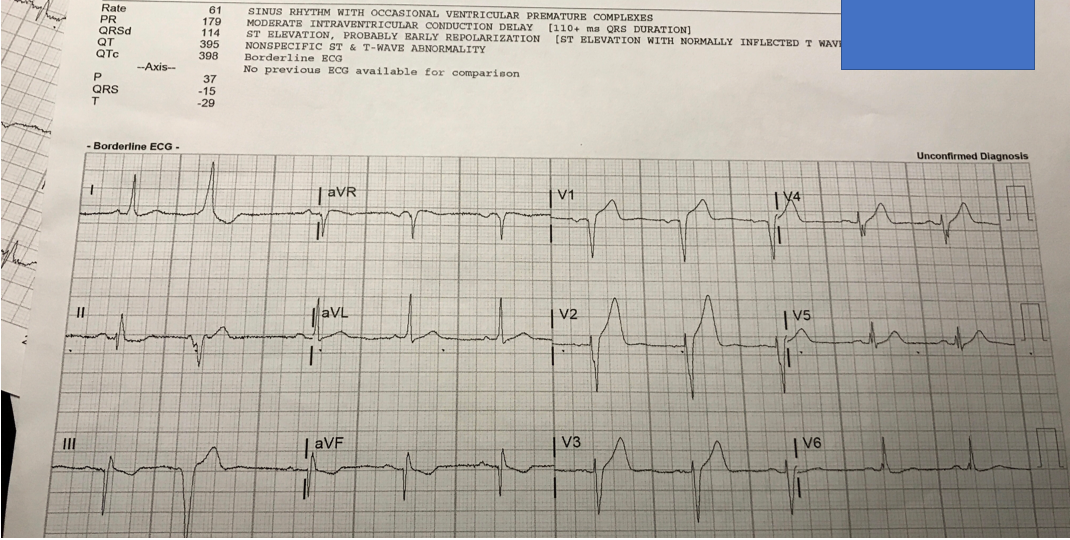
| Figure-1: The initial ECG in this case, obtained in the ED on this patient with chest pain. I’ve copied the computerized interpretation of this tracing (See text). |
=================
Thought #1:
- I would wager that the Emergency physician who read the ECG in Figure-1 did not use a Systematic Approach. If he/she did — they would surely have noticed that in addition to lead V2 (which as per Dr. Smith — shows an obviously much-taller-and-fatter-at-its-base-than-it-should-be, therefore hyperacute T wave) — there is NO way that lead V1 can be “normal” in a patient with new-onset chest pain. There is at least 2 mm of ST elevation in lead V1 (RED arrow) — and that is virtually never “normal”.
- There are many systems in use for ECG interpretation. Regardless of whether you use mine, or another one that you prefer — the KEY is to always go through each of the essential parameters to assess in the identical sequence, so that you never forget to assess them all. This entails looking at each of the 12-leads on the ECG.
- Advantages of Using a Systematic Approach: i) With just a little bit of practice — it will speed up your interpretation! (because you have a step-by-step approach — and will no longer go back-and-forth to reassess things you’ve already looked at); and, ii) A systematic approach will improve your accuracy (because you no longer leave things out …).
My SYSTEM: ( — CLICK HERE — )
Beginning with Descriptive Analysis:
- Rate & Rhythm — The rhythm is sinus at ~60/minute. There is one late-cycle PVC ( = the 2nd beat in the tracing).
- Intervals — The PR interval is normal; the QRS complex is not wide; and the QTc is not prolonged.
- Axis — There is a slightly leftward frontal plane axis (the QRS is all positive in lead I — and probably a little more negative than positive in lead aVF).
- Chamber Enlargement — None.
- Q-R-S-T Changes — There is a Q wave in lead aVF. We only see 1 sinus-conducted beat in lead III — and it’s hard to be certain if there is or is not a tiny initial r wave in this lead. There definitely is a small initial r wave in lead II. Otherwise there is a QS complex in lead V1 — but definite precordial lead R waves have formed by V2. R Wave Progression — shows slightly delayed transition (the R becomes taller than the S wave is deep between lead V4-to-V5). ST-T Waves — There are sagging ST segments in each of the inferior leads. The most remarkable finding is the ST elevation in leads V1 and V2 (and probably also a small amount in lead V3) — with T waves that look taller-and-fatter-than-they-should-be given relative amplitude of the QRS complex in leads V1-thru-V4.
Putting this Together in your Clinical Impression:
- The rhythm in Figure-1 is sinus at ~60/minute — there is 1 late-cycle PVC — and, there is evidence of a probable prior inferior MI (ie,a Q in lead aVF [if not also in lead III] — but with inferior lead ST-T waves that do not look acute). Of most concern — there is ST elevation in V1 & V2, and hyperacute T waves in leads V1-thru-V4. Given that this man in his 60s has new-onset chest pain — one has to assume an acute cardiac syndrome (presumed OMI) until you prove otherwise.
- P.S. — QRS complexes are fragmented (at least in leads V4, V5 and V6) — which strongly suggests there is underlying heart disease.
=================
Thought #2:
- Think “Patterns of Leads”. The experienced interpreter saves time and increases accuracy by “taking in” several leads in a given lead area at the same moment in time. For example, the “theme” in the inferior leads is that there has been prior inferior infarction — even though there is definitely no Q wave for the sinus-conducted beat in lead II. And, the reason I think there is slight ST elevation with a hyperacute T wave in lead V3 — is that there is NO doubt about these findings in neighboring leads V1 and V2. This is why the T wave in the next neighboring lead ( = lead V4) is probably also hyperacute (taller-and-fatter-than-it-should-be given the small QRS complex in V4).
=================
Thought #3:
- What about the Computerized Interpretation? It is hard to believe that the computer is calling chest lead ST-T waves in Figure-1 “probable early repolarization”. This just goes to show How Wrong the computer can be! But we should never be depending on the computerized interpretation to begin with!
- I happen to like computerized ECG interpretations — because I know how best to use them (CLICK HERE — for My Approach for Using the Computer). I realize many clinicians do not like computerized interpretations. It’s a matter of personal preference and clinical experience with computerized interpretations.
- The BASICS: Never look at the computerized interpretation until after you have made your own independent assessment! In general — the computer is great for calculating rates, axis, and intervals. In my experience — it is terrible for assessing any rhythm other than sinus! The computer usually does OK for assessing normal tracings — but it may overlook certain findings (such as the ST elevation and hyperacute T waves, as well as the prior inferior MI in Figure-1). BOTTOM Line: The computerized report may help by suggesting certain findings that you may not have thought of — BUT — you must always overread what the computer says. IF you disagree with what the computer says — then cross out those parts in the computer report that you disagree with! In this particular case — I suspect that the computer reading of, “probably early repolarization” may have led one or more of the clinicians astray …
![]()