Medics were called to see a 20-something type 1 diabetic with h/o DKA who had altered mental status.
He was found to have “Kussmaul” respirations and respiratory distress.
He was not in shock, his blood pressure was adequate, and pulses were strong.
He was put on the cardiac monitor:
 |
| Regular wide complex tachycardia. |
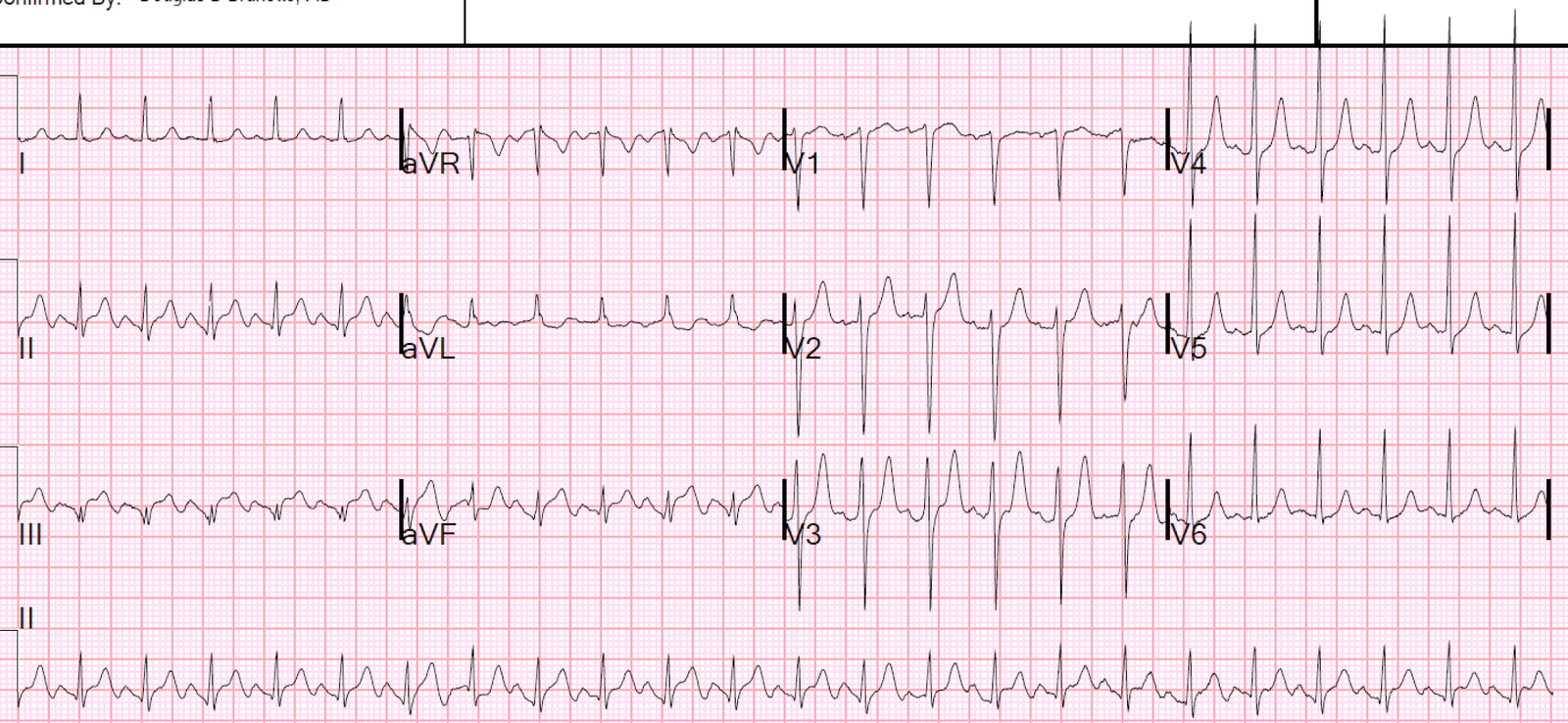
A 12-lead ECG was recorded:
 |
| Regular Wide complex tachycardia at a rate of 200. What do you think? If you’re the medic, what would you do? |
Whenever there is a wide complex, especially in a patient with DKA, one should think of hyperkalemia (sinus rhythm, often with “invisible P-waves”).
However, this rate is too fast for sinus tach and the morphology is not right for hyperkalemia. Still, calcium is harmless and it is harmless to give 3 grams of calcium gluconate.
He arrived in the ED in the same condition. He was hemodynamically stable but with altered mental status and respiratory distress. Cardiac echo showed hyperdynamic performance. Blood gas showed severe acidosis, with pH 7.00, pCO2 25 and HCO3 of 6. K retured at 4.5 mEq/L.
He was treated with calcium, bicarbonate, and magnesium. He was intubated.
He had this ECG recorded:
 |
| What do you think? What do you want to do? Suppose the patient did not have altered mental status from DKA and was not intubated? |
Analysis: VT vs. SVT with aberrancy vs. sinus tachycardia with hidden P-waves. (With a rate this fast, and no inkling of P-waves, sinus is very unlikely but if you were not sure, you could record Lewis Leads.)
This ECG is almost certainly supraventricular tachycardia with aberrancy. Why?
First: pretest probability
The patient is young and without heart disease
Good LV function makes VT less likely (except for fascicular VT)
Second: the ECG itself:
1. There is an inferior axis. The impulse originates cranially and propagates caudally. In contrast, VT, because it originates in the ventricle, which is lower left, generally propagates toward the upper right.
2. More importantly, there is a typical right bundle branch block (RBBB) morphology:
a. There is RR’ in V1 and the R’ is larger than the R.
b. There is a rapid, narrow R-wave in V5 and V6, with a wide S-wave.
This latter makes SVT with RBBB aberrancy almost certain.
Thus, it is very likely that it will convert with adenosine. The medics could have given adenosine and converted. Since the patient was hemodynamically stable, there was no rush to convert and therefore it is OK that they left it alone.
If you’re wrong and give adenosine to a patient with VT, don’t worry. Adenosine has been shown to be safe in Ventricular Tachycardia and is even recommended now in ACLS.
Of course, electrical cardioversion will work very well but generally requires sedation unless the patient is already obtunded. This patient was intubated and sedated, so electricity is easy to use.
However, if this patient were not so sick with DKA that he needed to be intubated, adenosine would be the treatment of choice.
The patient was diagnosed with VT and electrically cardioverted.
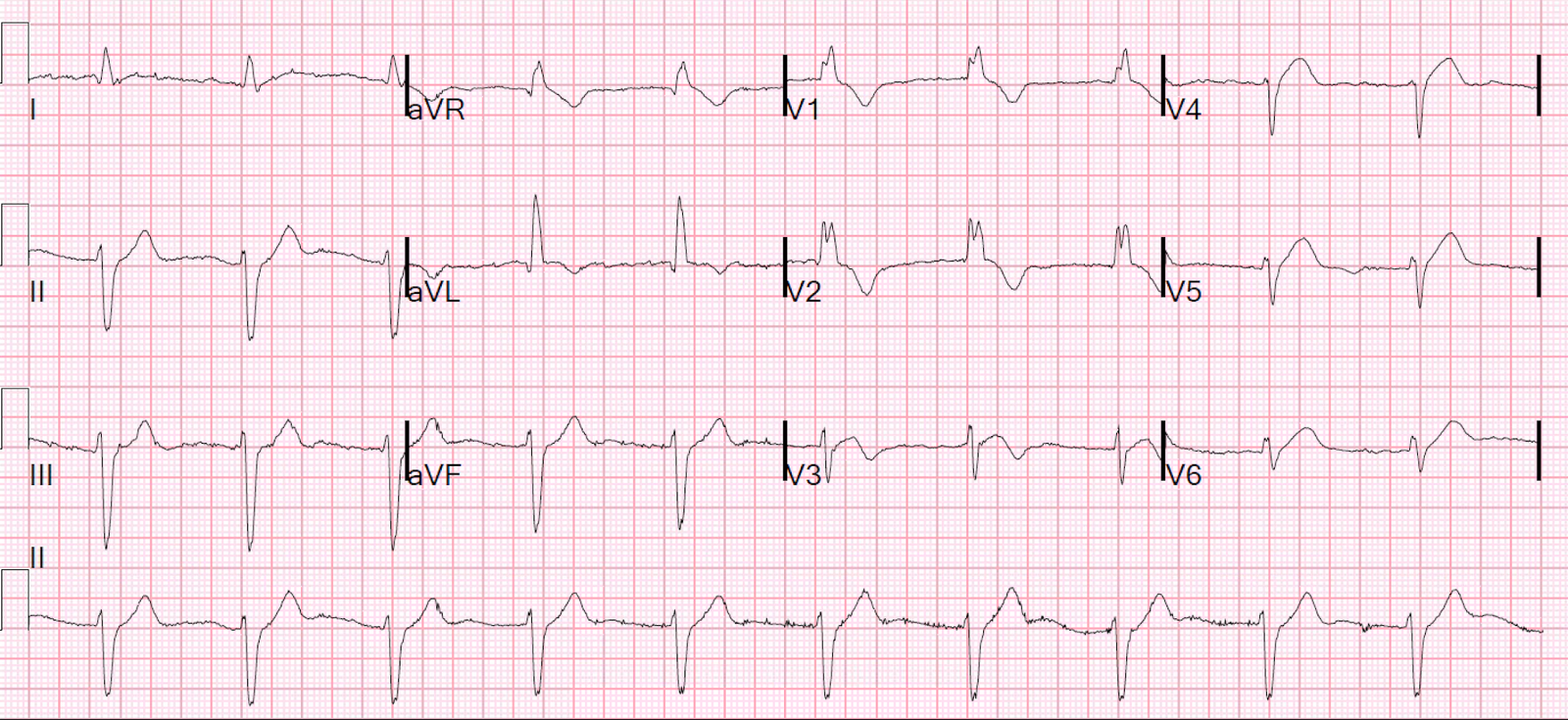
Here is the post-cardioversion ECG:
 |
| Sinus Tachycardia with normal QRS and axis and nonspecific ST-T abnormalities |
There is no baseline RBBB. The right bundle generally has a longer refractory period than the left bundle, so that when there is a fast rate, it can result in RBBB aberrancy.
The patient did well and was later diagnosed with SVT with aberrancy.
Learning Points:
1. Adenosine is safe in regular wide complex tachycardia. (But NOT in irregular polymorphic wide complex tachycardia, as this could be WPW with atrial fib)
2. If there is typical RBBB morphology, it is almost certainly SVT with aberrancy. There are also fairly rare fascicular ventricular tachycardias which can mimic SVT with aberrancy. However, you won’t hurt them with adenosine.