A 40-something man with h/o asthma presented with cough, sore throat, earache, shortness of breath and chest tightness. His wife had similar symptoms, but without the SOB.
The patient received albuterol with some relief. He was being set up for discharge when the provider decided it would be a good idea to record an ECG. Here it is:

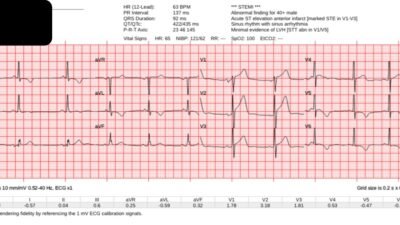
The conventional Veritas computer interpretation was:
ST ELEVATION, CONSIDER ANTERIOR INJURY [MARKED ST ELEVATION W/O NORMALLY INFLECTED T-WAVE IN V2-V5]
***ACUTE MI***
What do you think?
= = =
= = =
= = =
= = =
I was shown this later, and thought it represented LAD OMI, with Hyperacute T-waves in V2 and V3. Moreover, it even meets STEMI criteria in V2 and V3, with more than 2 mm in each of V2 and V3)
The providers also thought so at the time. I ran the EKG through the Queen and this is what I got:

New PMcardio for Individuals App 3.0 now includes the latest Queen of Hearts model and AI explainability (blue heatmaps)! Download now for iOS or Android. https://www.powerfulmedical.com/pmcardio-individuals/ (Drs. Smith and Meyers trained the AI Model and are shareholders in Powerful Medical).
If we use the 4-variable formula, the value returns at 17.1, which is below the optimal cutoff of 18.2, and very convincing for “early repolarization” (normal variant ST Elevation). A large reason for that is the relatively short QT interval (the computer measured it at 379 ms; most LAD OMI have a QT interval longer than 400ms. (The formula uses the Bazett correction, but here the heart rate is 60 and needs no correction; do not correct if the heart rate is below 60)
The Queen measured the QT at 406 ms (not 379), and she uses the Fridericia correction, which gives a corrected QT of 403. If we use this for the 4-variable formula, then we get a value of 17.6, still below 18.2
I am not certain if they used the Queen or the formula or neither, but they did not activate the cath lab, and instead decided to wait for a troponin:
The first troponin was drawn 2 hours after arrival (25 minutes after the ECG was recorded) and returned 1 hour after the ECG at 23ng/L.
A 2nd ECG was recorded 47 minutes after the first, and was unchanged.

Again, the Veritas conventional algorithm gives:
ST ELEVATION, CONSIDER ANTERIOR INJURY [MARKED ST ELEVATION W/O NORMALLY INFLECTED T-WAVE IN V2-V5]
***ACUTE MI***
A 2nd troponin was collected 4 hours after arrival (2.5 hours after the first ECG was recorded), and returned at 19 ng/L. This pretty convincingly rules out acute MI, although I would have obtained a 3rd troponin.
They gave him ibuprofen. The patient reported later that his pain was better leaning forward and worse leaning back. Due to this, they gave a diagnosis of “pericarditis”. I am skeptical of that.
Learning Points
- ECGs are hard. Normal Variant ST Elevation mimics LAD OMI, and vice versa.
- The PMCardio Queen of Hearts not only helps you recognize OMI that are not obvious, but helps you to avoid false positives. (We have data showing 75% decrease in false positive activations, to be presented in Madrid soon)
- The 4-Variable formula is also useful, but not as good as Queen of Hearts
= = =
======================================
MY Comment, by KEN GRAUER, MD (8/15/2025):
When I was in training — we were taught that if you were correct about the diagnosis of acute appendicitis more than 80% of the time — that this meant you were missing a lot of cases that should have been surgically explored to rule out acute appendicitis.
- This was of course long before ultrasound, CT scan and MRI became the commonly used modalities that have so greatly increased our diagnostic accuracy far beyond the modest 80% possible at that time period by history, exam, flat plat x-rays and CBCs.
= = =
How this Relates to Today’s CASE:
The point is that just because your best “Gold Standard” Test in the early 1980s did not correctly identify the diagnosis (ie, acute appendicitis on the basis of localized RLQ tenderness) — does not mean that it was wrong to surgically explore some patients patients who ended up not having acute appendicitis as the cause of their RLQ tenderness — OR — in the case of a patient who in 2025 presents with CP (Chest Pain) and a worrisome ECG, that it is “wrong” to activate the cath lab in order to rule out an acute coronary occlusion in some patients who end up having normal coronary arteries on cath. When you are appropriately concerned — better to be prudent than to delay or entirely overlook an acute OMI.
- Although today’s patient was a relatively younger adult with a history of asthma (but no known coronary disease) — who presented with URI symptoms that his wife also had — this patient did have chest tightness.
- As a result, it was appropriate to order today’s initial ECG (that I’ve reproduced and labeled in Figure-1). This ECG was then appropriately interpreted by the treatment team as cause for concern — and, as a result — further evaluation of this patient was clearly indicated.
- Fortunately — results of 2 Troponins and a repeat ECG that showed no change compared to ECG #1 essentially ruled out acute MI — but it would not have been wrong to activate the cath lab IF any doubt had remained.
= = =
Today’s Initial ECG in Figure-1:
There are a number of interesting findings in ECG #1:
- The rhythm is sinus at ~60/minute. The PR interval is normal — the QRS is narrow — and as per Dr. Smith, the QTc is relatively short (ie, less than 400 msec.) — which is in favor of a more benign entity.
- The frontal plane axis is horizontal (close to 0 degrees, given the isoelectric QRS in lead aVF). There is no chamber enlargement.
- Importantly — R wave progression is normal, with no loss of anterior forces — and, with transition (where the R wave becomes taller than the S wave is deep) appropriately occurring between leads V3-to-V4.
- My “eye” was immediately drawn to the disproportionately “hypervoluminous” ST-T waves in leads V3,V4 (within the RED rectangle) — that in a patient with CP, has to suggest a hyperacute change until we have evidence to the contrary.
- In support of this concern is the ST-T wave appearance in neighboring lead V4, which shows some ST elevation in association with a larger-than-expected ST-T wave.
- On the other hand — the ST elevation in leads I and aVL is clearly concave up (ie, “smiley”-configuration) — in association with the prominent J-point notching that is so often associated with repolarization variants.
- Finally — there are surprisingly multi-notched (fragmented) QRS complexes in both leads III and aVF (an rSR’S’ complex in III — and an rs-slurred-R’S’ complex in aVF). This makes for a very unusual QRS morphology for a 40-something adult whose prior medical history had been remarkable only for asthma.
= = =
My Thoughts:
My hunch on reading about this case and seeing the initial ECG in Figure-1 — was that this tracing was a “fake” and not indicative of an acute cardiac event.
- As concerning as the ST-T wave appearance in leads V2,V3,V4 was — the QTc is relatively short, R wave progression is normal (with no loss of anterior forces) — and the ST-T wave appearance in leads I and aVL suggests this may all be a repolarization variant.
- In addition — there is no reciprocal ST depression in inferior leads II and aVF — and the shallow T wave inversion in lead III is not necessarily ischemic given the multi-fragmented isoelectric QRS complex in lead III. That said — I was in no way certain this was all benign solely from this initial ECG.
- I agree with Dr. Smith that obtaining a 3rd Troponin value would have been advisable (We’ve seen cases of acute OMI in which the first 2 Troponin values were not abnormally increased).
- As we’ve often emphasized — “Acute Pericarditis” is a greatly overused diagnosis not justified solely on the basis of “pain better leaning forward and worse leaning back” (especially not without chart documentation of having at least carefully listened to the heart for a pericardial friction rub — See My Comments in the June 11, 2022 post and the June 8, 2022 post).
- In my opinion — an Echo should be part of this patient’s initial evaluation (to ensure no underlying structural heart disease) given more fragmentation than you probably have ever seen in leads III and aVF in this relatively younger adult being worked up for CP and an initial ECG with potentially hyperacute anterior T waves.
= = =
Figure-1: I’ve reproduced and labeled the ECG in today’s case.