
This was sent by a Saleh Hatem, an avid reader of the blog.
The patient presented with chest pain:
 |
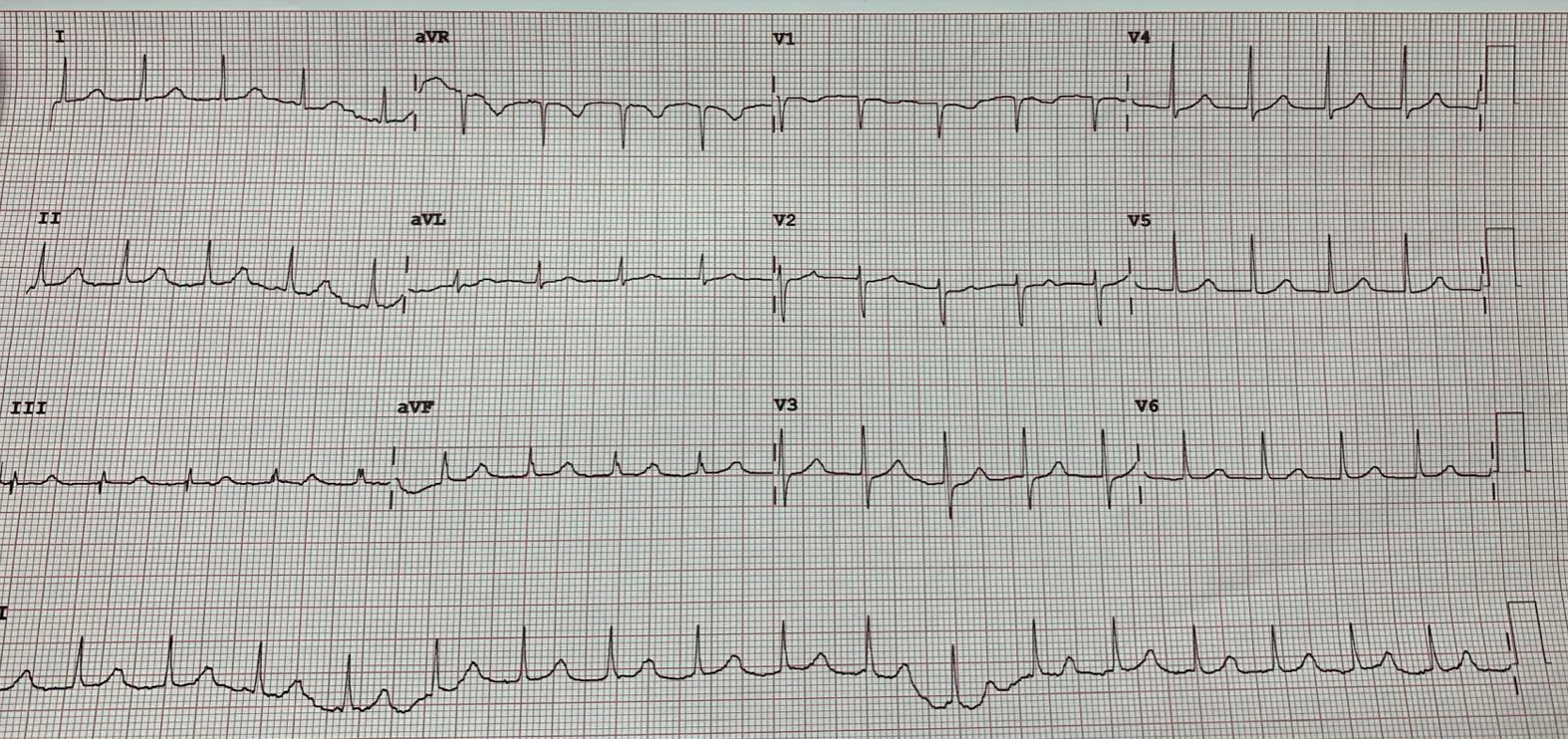
| ECG #1: There is a narrow complex tachycardia.
Is there inferior ST Elevation? |
Here was my interpretation:
What appears to be ST Elevation in inferior leads is really a P-wave that is contiguous with the QRS. (The next bump over is a T-wave that looks like a P-wave!).
Since the P-wave is not inverted, it is NOT retrograde, and therefore it is a native sinus beat. This sinus beat does conduct, but there is severely prolonged PR interval (severe first degree AV block), with a PR interval of over 400 ms.
So: Sinus tachycardia with severe first degree AV block.
Here is what he wrote:
Her serial trop was negative.
Later ECGs confirmed your interpretation, Dr. Smith. Thanks.
The reader later sent these same followup ECGs:
 |
| ECG #2: The sinus rate has slowed and now the P-wave is hidden in the T-wave. |
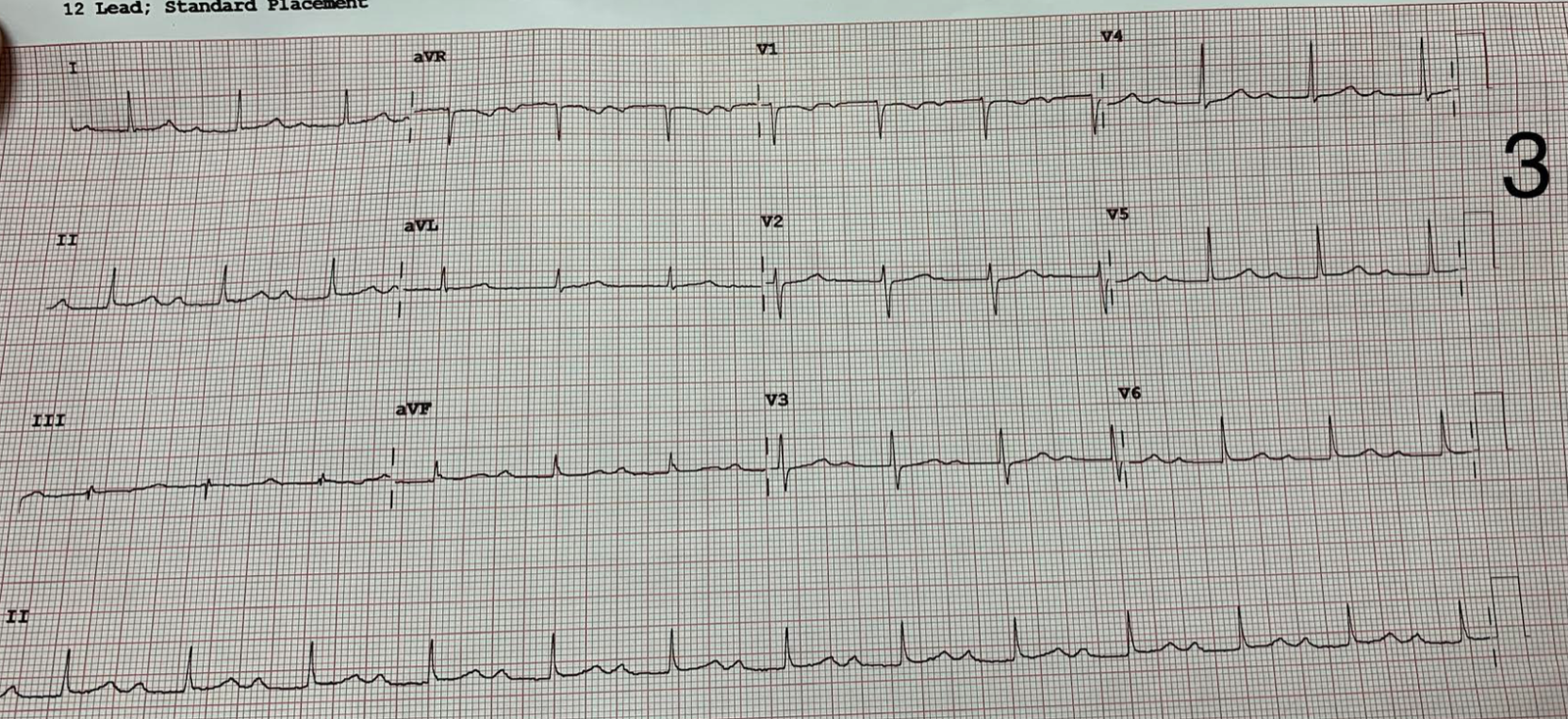 |
| ECG #3: The sinus rate has slowed even more and now the P-wave comes after the T-wave, with a PR interval of just under 400 ms. |
![]()
===================================
MY Comment by KEN GRAUER, MD (3/1/2020):
===================================
This is an insightful case succinctly explained by Dr. Smith. For the purpose of academic discussion — I will expand on a number of important points.
- For clarity — I have reproduced and labeled the ECG in this case in Figure-1. (Please NOTE — I wrote my comment before the reader sent in the 2 follow-up tracings in this case = ECGs #2 and #3).
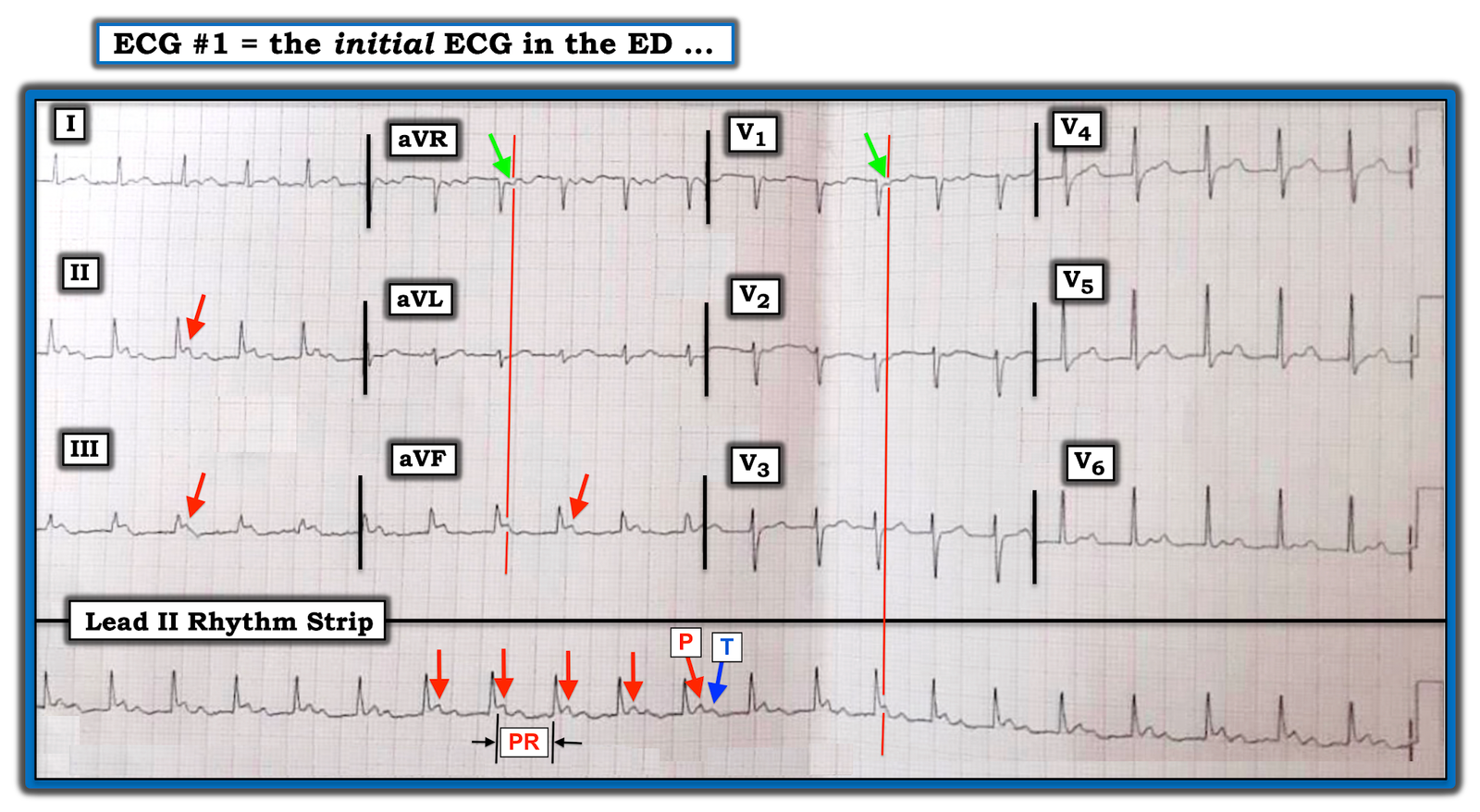 |
| Figure-1: The ECG sent to Dr. Smith by a reader. The patient presented with chest pain. Presumably, this is her initial ECG obtained in the ED (See text). |
MY THOUGHTS: Despite my best efforts to straighten this tracing — it is both angled and folded, and this distorts measurement of intervals.
- Cell phone pictures of ECGs have become an invaluable tool for quick delivery of acute tracings to others for timely expert consultation. That said — it is important to remember that folding and angling of a tracing will distort ECG grid lines. Inability to reliably measure intervals because of this distortion may greatly impair accurate interpretation of complex arrhythmias. For Example — In Figure-1, the reason my caliper measurement of the PR interval varies is not because the PR interval is increasing — but because this tracing is slanted!
- As per Dr. Smith — the underlying rhythm in Figure-1 is sinus tachycardia, with marked prolongation of the PR interval (I measure a PR interval ~2 large boxes in duration = 0.40 second). I’ve marked a number of P waves with RED arrows — whereas the T wave in the long lead II rhythm strip is highlighted by a BLUE arrow.
- As per Dr. Smith — the polarity of each P wave is what tells us that P waves (RED arrows) are conducting forward with a very long PR interval, rather than backward in retrograde fashion. Thus, P waves are upright in each of the 3 inferior leads (RED arrows) — and negative in right-sided leads aVR and V1 (GREEN arrows), as is commonly seen with forward-conducting sinus P waves.
- I believe the R-R interval in Figure-1 is constant — although this is not easy to determine because of the aforementioned distortion of the ECG grid. The reason I KNOW that the PR interval is not increasing in this tracing — is that the distance from each P wave in the long lead II rhythm strip — to the preceding QRS complex (ie, the QRS complex behind it) remains the same.
- The rate of the sinus tachycardia in Figure-1 is extremely fast = about 130/minute! So, my 1st, 2nd and 3rd questions about this patient would be WHY is her heart rate so fast?
Finally — We should ask, WHY is the PR interval so long?
- Most of the time with sinus tachycardia the PR interval decreases. We are not privilege to any information about this female patient beyond that she presented with chest pain — and was found to have negative serial troponins. I can’t remember the last time I saw a tracing with sinus tachycardia this fast — and a PR interval this long. Therefore — I’d LOVE to know more about the clinical history and follow-up in this case.
- PEARL — I found a short-and-sweet Review regarding 1st-Degree AV Block by Oldroyd and Makaryus (CLICK HERE). Among the Common Causes of 1st-Degree AV Block listed in this brief Review (to which I added some + suggestion from Dr. Jerry Jones in Comments below) are: i) increased vagal tone (especially common in younger individuals with athletic training); ii) Fibrotic changes of the cardiac conduction system (especially in older patients); iii) Coronary artery disease (including Acute MI); iv) Inflammation/infection (presumably myocarditis; rheumatic fever; endocarditis; etc.); v) Infiltrative disease; vi) Lyme disease with carditis; and, vii) Neuromuscular disorders.
- P.S. — We are told that “later ECGs confirm the impression that the rhythm is sinus tachycardia with 1st-degree AV block”. I’d LOVE to see those later ECGs. Was this patient in sinus tach with a very long 1st-degree block — or — Was the rhythm in Figure-1 really ATach (Atrial Tachycardia), in which the PR interval can be short or long depending on where the atopic atrial activity originates?
- FOLLOW-UP Note (3/4/2020): My wish was granted! After I posted the above comment — the reader sent us ECGs #2 and #3, which were the follow-up tracings in this case (See the end of Dr. Smith discussion above). As per Dr. Smith — as the heart rate slowed down, confirmation that the PR interval was indeed unchanging (ie, ~0.40 second) became evident — which proves the diagnosis of 1st-Degree AV Block (and rules out Mobitz I with a long Wenckebach cycle; and also rules out Atrial Tachycardia as a possibility). This leaves to be determined: i) Why the patient presented in such a rapid Sinus Tach (ie, ~130/minute); and, ii) Why this patient has such a markedly prolonged PR interval. Our THANKS to Dr. Smith and the reader for presentation of this case!
![]()


