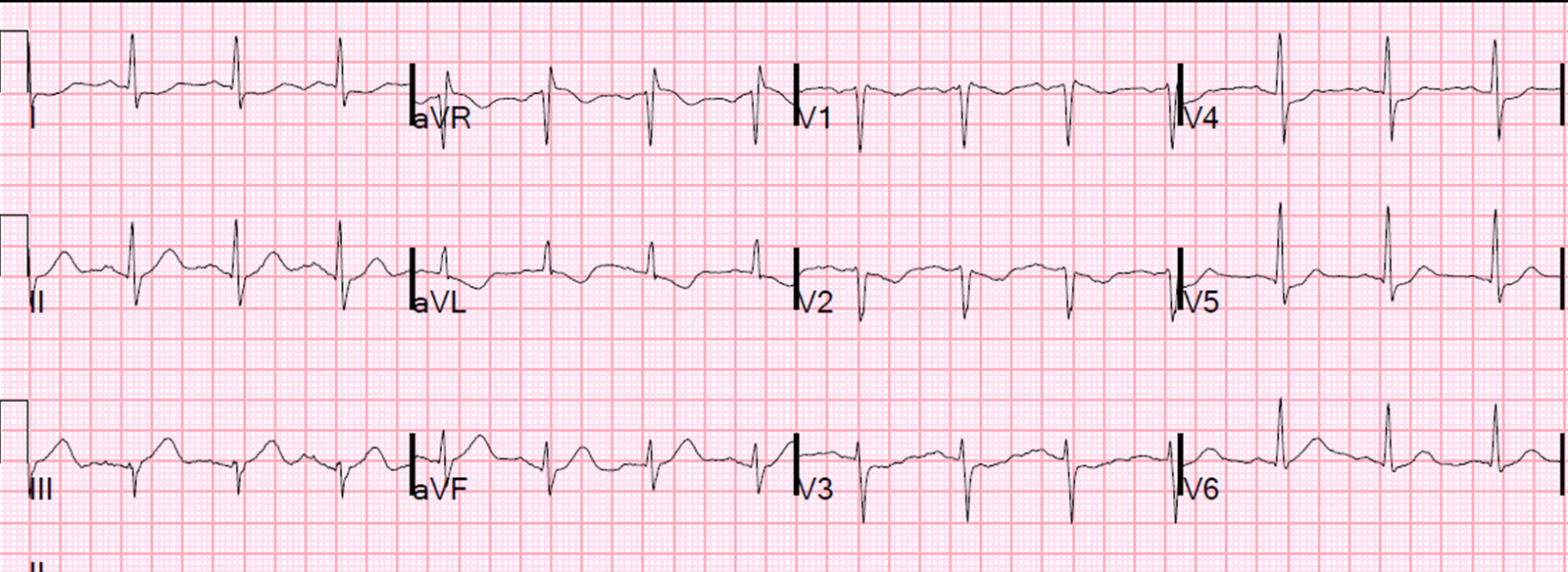
A 50 something with no past history presented with sudden severe substernal chest pain with no radiation or associated symptoms. The clinicians were very impressed with his presentation and were sure he was having an MI. Here is his initial ECG:
 |
| Not very revealing. They had expected a positive ECG. |
A chest x-ray was completely normal.
The first troponin was negative.
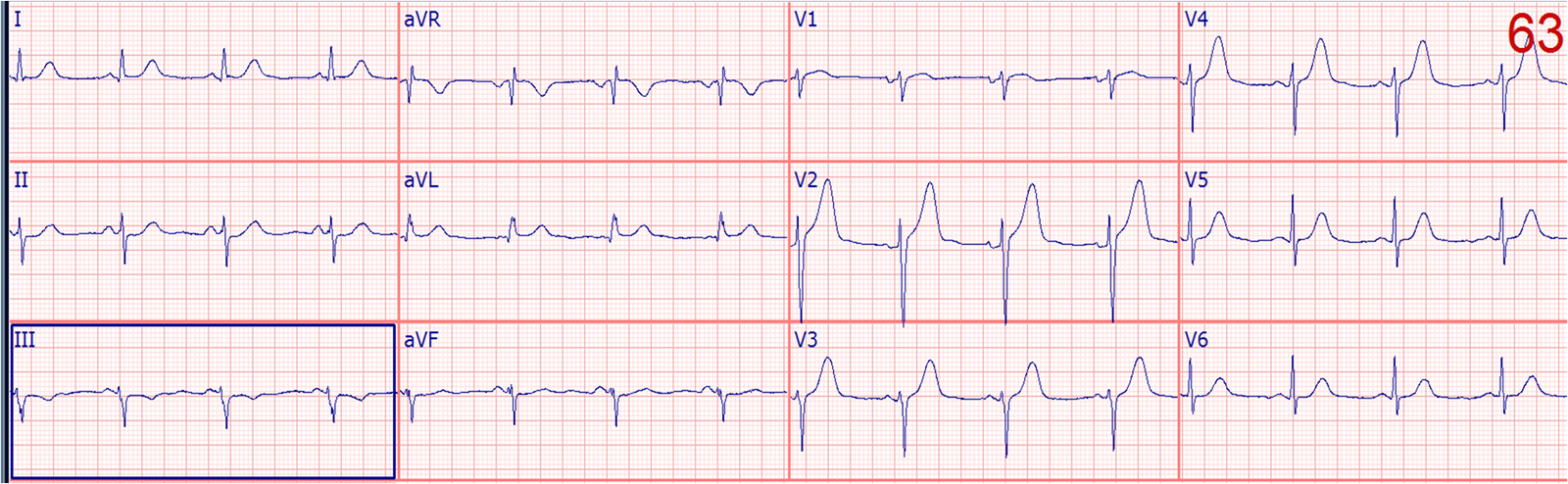
The pain persisted and another ECG was recorded 80 minutes later:
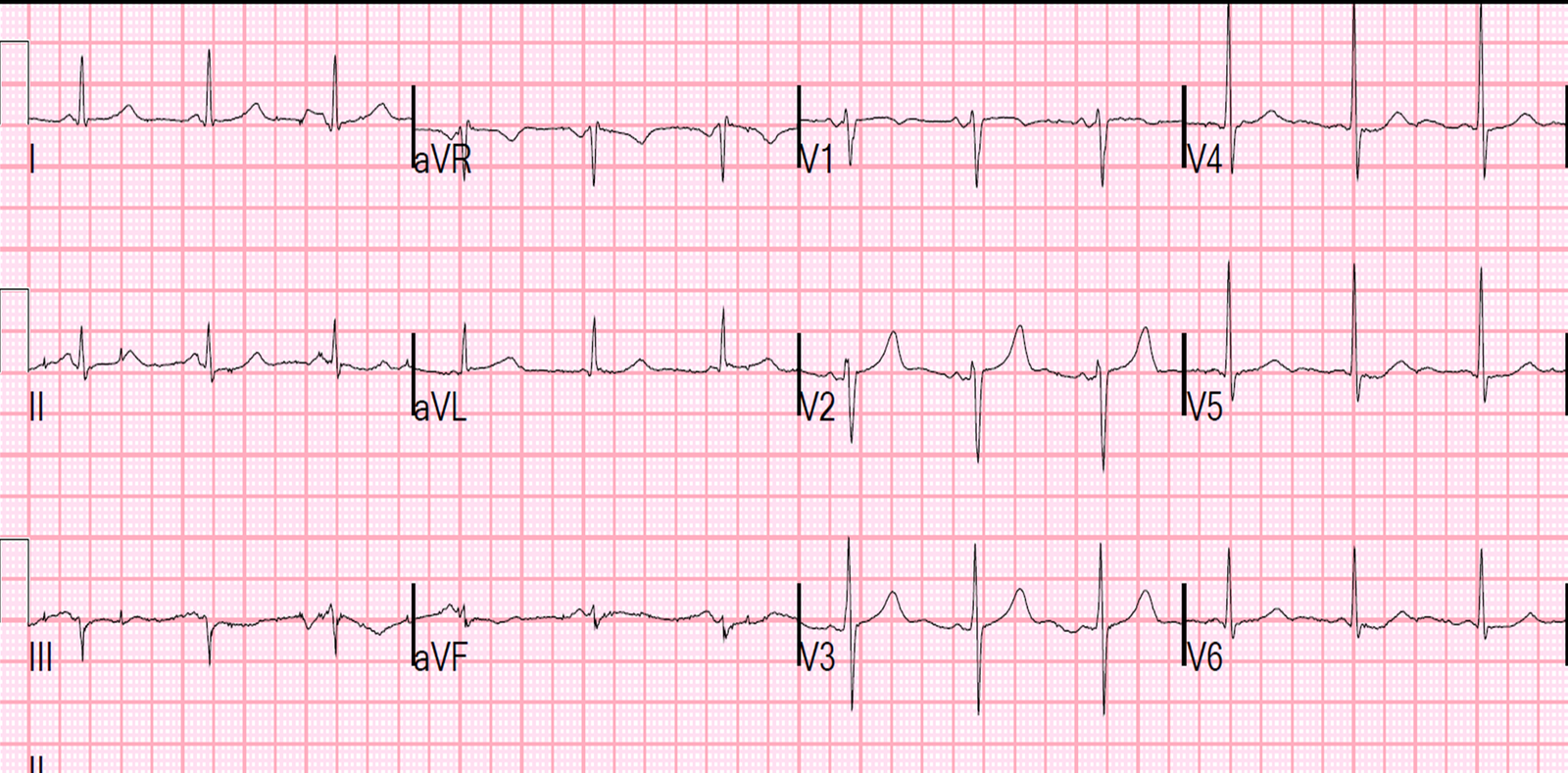 |
| There is now some nonspecific ST depression in V5 and V6. |
The second troponin returned negative at 5 hours. The patient’s pain persisted.
The clinicians were certain that something serious was wrong and were not convinced by the ST depression that it was ACS, so they performed a bedside ultrasound.
Here is the parasternal short axis:
There is good function and normal wall motion
Here is the parasternal long axis:
The emergency physician thought he saw a flap in the aorta (the echo free area behind the left atrium (see still image with arrow below):
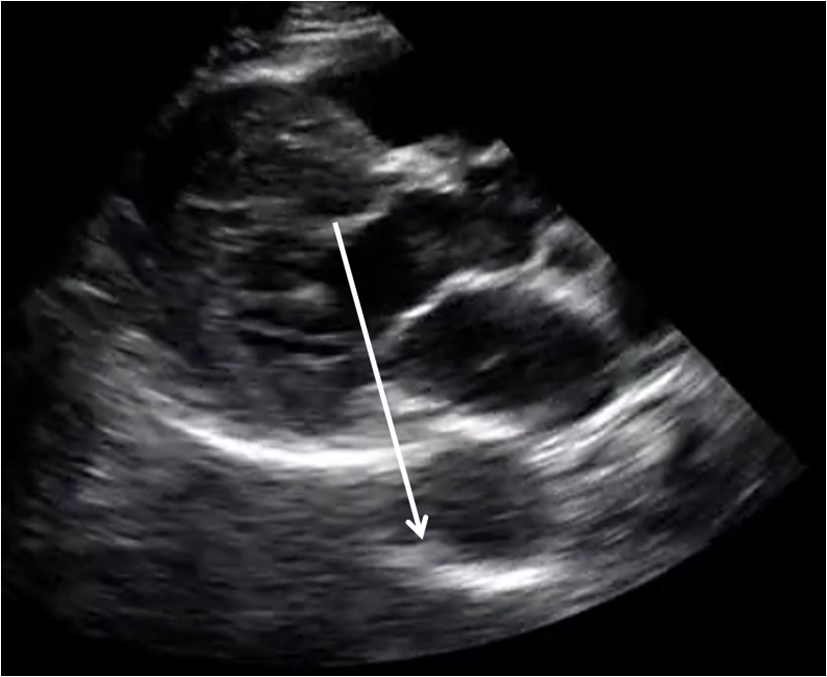 |
| The arrow points to something that, on the video, is apparently moving inside the aorta on the video |
So the emergency physician took a look at the aorta through the suprasternal notch:
You can see a flap in the aorta
Here is a still picture with arrows pointing to the flap:
 |
| Here you can easily see the flap |
Here is the CT scan:
 |
| Here you can clearly see the dissection flap |
He went to the operating room and had a successful graft placed. As I understand it, he was not a candidate for intravascular stent placement.
Learning point:
I don’t usually do an ED ultrasound on every chest pain patient. Maybe one should. But in this case there were clues that something was wrong:
1. Sudden pain
2. Never had before
3. Looked ill and in distress
4. Could not be explained by the ECG
5. Troponins negative.
One could argue that this could simply be suspected and he could get a d dimer, the CT if positive, or simply go straight to CT.
Fair enough.
But this is an easy screening test that one could do on more patients with unexplained chest pain.