Written by Magnus Nossen
A man in his early 30s was found unresponsive in bed by his wife. She immediately initiated CPR. Upon arrival, emergency medical services found the patient in V-fib. ROSC was achieved after approximately 15 minutes of resuscitation. The patient remained unresponsive and was intubated. The following ECG was recorded post-ROSC.
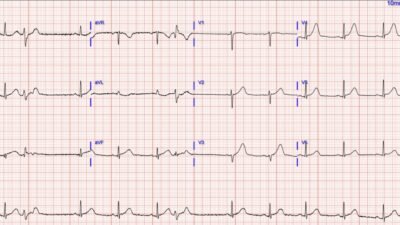
ECG #1
ECG recorded in the ambulance after return of spontaneous circulation. The ECG shows atrial fibrillation with atypical ST elevation in leads V2–V6, I and aVL.
Smith: there are bizarrely prominent J-waves in II and aVF. There are what resemble hyperacute T-waves in I, aVL, and V2-V6, with a lot of ST Elevation, and also reciprocal STD in III and aVF. One must always be a bit skeptical if the ECG is recorded IMMEDIATELY after ROSC, as the low flow state can result in an OMI appearing ECG even when there is no OMI. Unless there is no doubt, I recomment waiting 10-15 minutes to record again.
Case continued:
The patient remained stable during transport to the ED with no further V-fib episodes. He arrived intubated with ongoing adrenalin infusion to maintain adequate MAP.
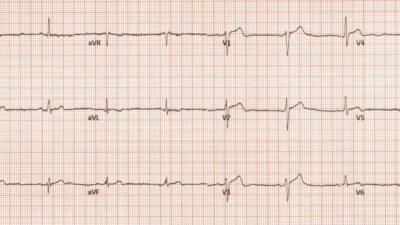
ECG recorded on admission (ECG #2)
The admission ECG had poor quality. Here the PM cardio App has been used for image optimalization. There is now SR and non-specific ST-depression in the inferior leads. This ECG was recorded about 45minutes post ROSC with ongoing adrenalin infusion that may have contributed to the non-specific ST-depression inferiorly.
Smith: as suspected, the OMI findings have largely disappeared. So this could either be a reperfused OMI or a case in which the low flow state mimicked OMI. In either case, it is very reasonable to go to the cath lab.
Echocardiography performed bedside in the ED showed normal systolic function and no wall motion abnormality. Smith: this makes OMI less likely, depending on the quality of the images and expertise of the sonographer.
Case continued: Due to V-fib and atypical STE after ROSC, an angiogram was done which did not show any sign of atherosclerosis or coronary artery spasm. Further evaluation with CT excluded aortic pathology, pulmonary embolism, and cerebrovascular accident. Serum electrolytes were within normal limits.
Troponin T on admission was 349ng/L and peaked at a modest 619ng/L. This troponin value post-ROSC does not give any indication of the cause of cardiac arrest as values in the hundreds can occur from cessation of coronary flow due to the cardiac arrest itself.
The patient was admitted to the cardiac intensive care unit (CICU) without a clear cause of the arrest.
The next day, while in the CICU, dynamic ECG changes were observed on continuous 12‑lead monitoring, culminating in an in‑hospital cardiac arrest. A 12‑lead ECG leading up to the cardiac arrest (ECG #3) is shown below followed by Fig #1 which compares the precordial leads from ECG #2 (on admission) and ECG #3 (prior to arrest)
These tracings show subtle but important clues to the diagnosis and the underlying cause of this patient’s cardiac arrest. Enlarge the images and look closely. What might be the cause of the cardiac arrest?
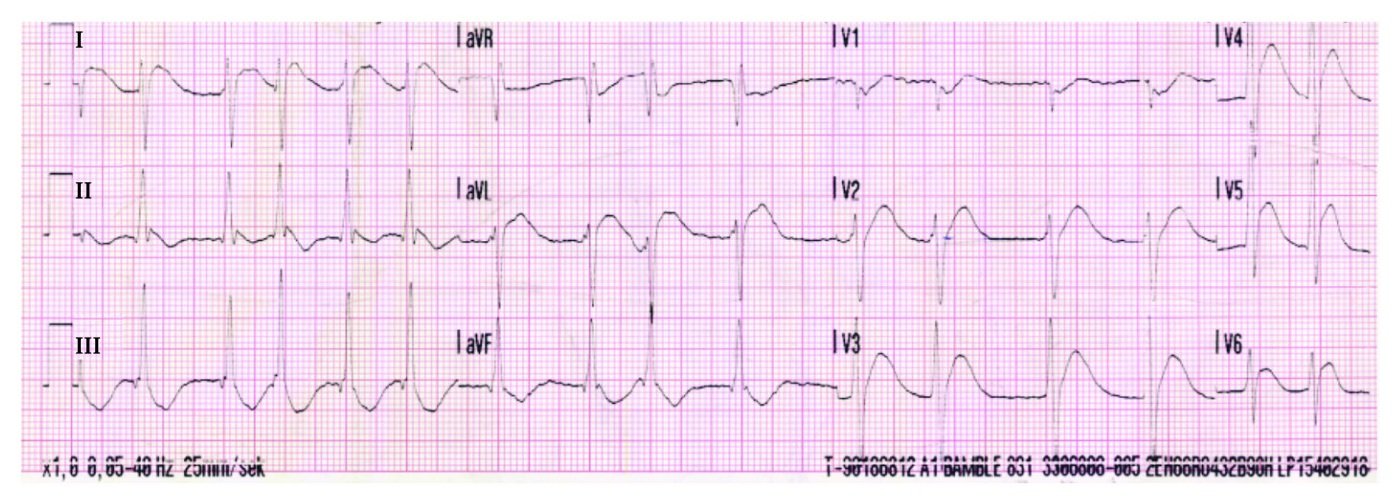
ECG #3
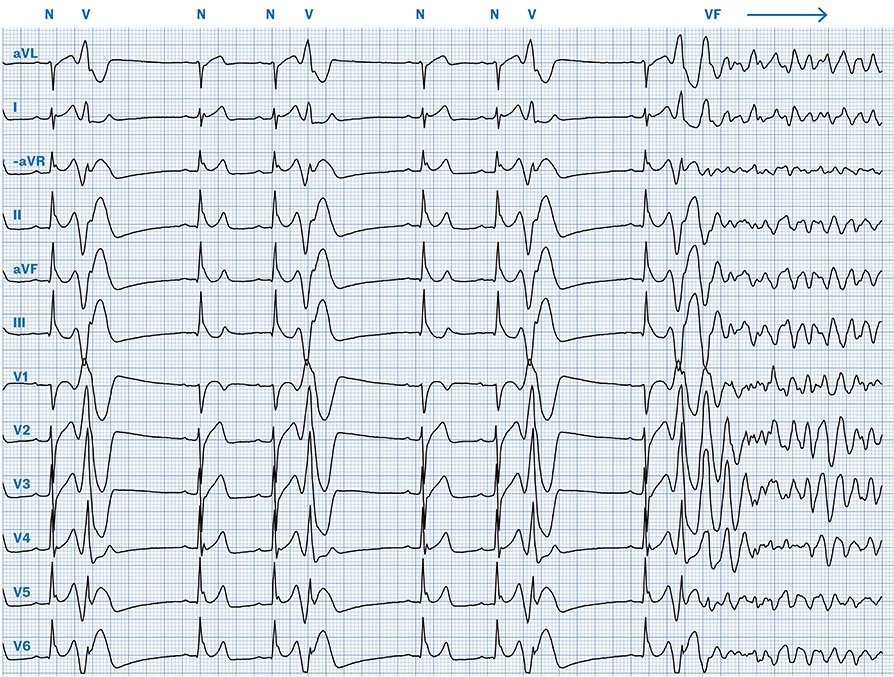
ECG immediately before cardiac arrest (Cabrera format, paper speed 25 mm/s). Sinus rhythm, rate 65 beats per minute. The sinus beats (labelled N) show a vertical axis and narrow QRS complexes. The PR interval is normal (174 ms), as is the corrected QT interval (414 ms), and there are no ischaemic ST-segment or T-wave changes. Frequent unifocal premature ventricular complexes (PVCs, labelled V) are present, occurring with a relatively short coupling interval (400 ms) and coinciding with the T wave (R-on-T phenomenon). Distinct J waves are visible in the inferior and lateral leads. Towards the end of the tracing, an R-on-T PVC triggers ventricular fibrillation (labelled VF).
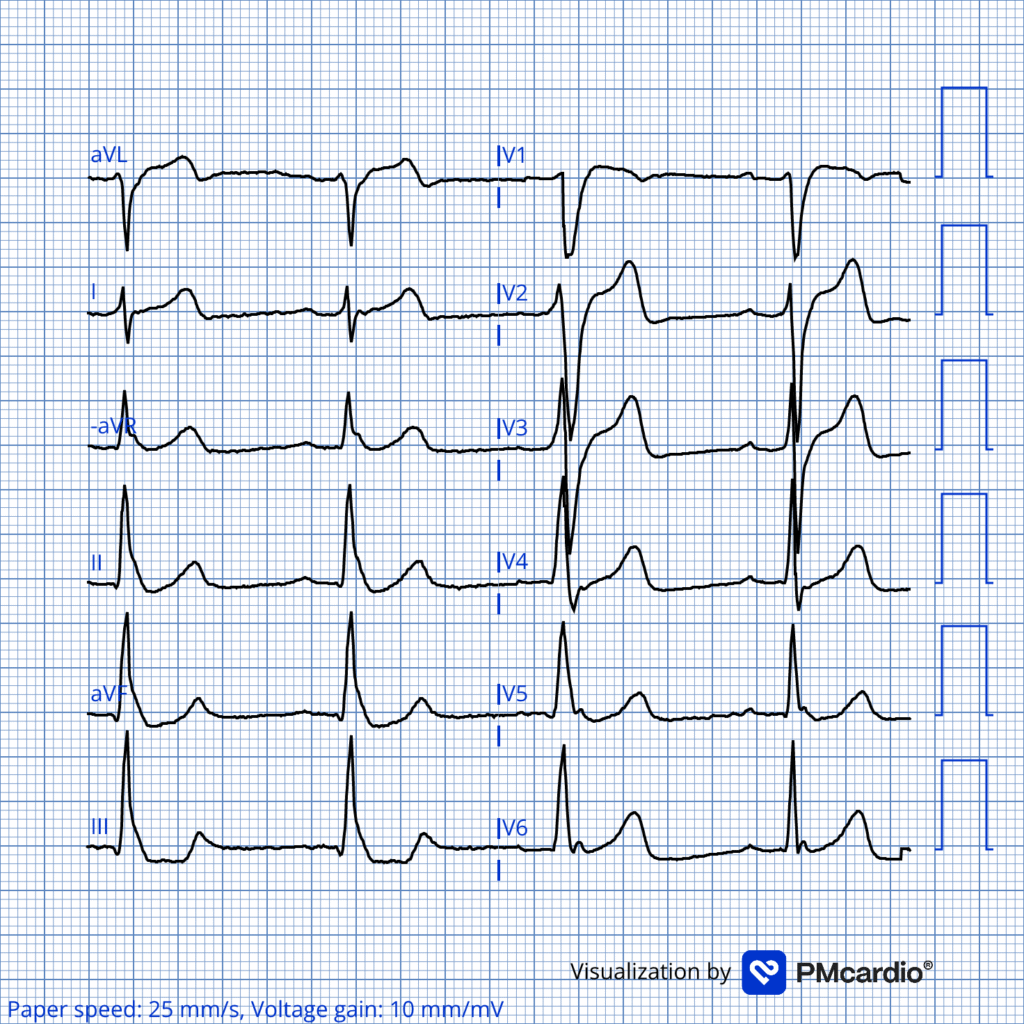
Fig #1
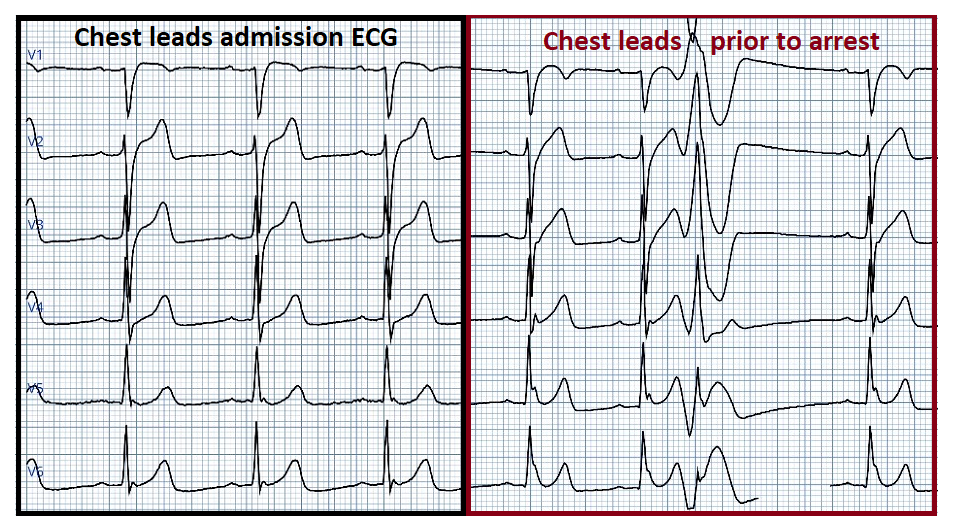
Chest leads on admission (left) compared to chest leads prior to cardiac arrest which occured the day after admission. Notice the widespread distribution and markedly changed amplitude of J waves prior to cardiac arrest!
Discussion:
This patient was diagnosed with Early Repolarization Syndrome (ERS). ERS is an arrhythmia syndrome in which early repolarization pattern on the ECG is associated with malignant ventricular arrhythmias or sudden cardiac arrest. It is essentially the “malignant” subset of early repolarization. To make the diagnosis of ERS it is required to have Early Repolarization Pattern (ERP) in a patient with documented polymorphic VT or ventricular fibrillation and a structurally normal heart. Other causes of malignant arrhythmia must be ruled out to diagnose ERS (1). ERS is a diagnosis of exclusion which should not be arrived at without a thorough diagnostic work up. If an extensive work up does not provide any other apparent cause of PMVT or V-fib and the patient has ERP in the ECG — then ERS is diagnosed.
Early repolarization is VERY common and when found incidentally in asymptomatic individuals it does not warrant any further work up. ERP is defined by the presence of J-waves on the ECG (1). J waves have different morphologies as shown in Fig #2.
Fig #2
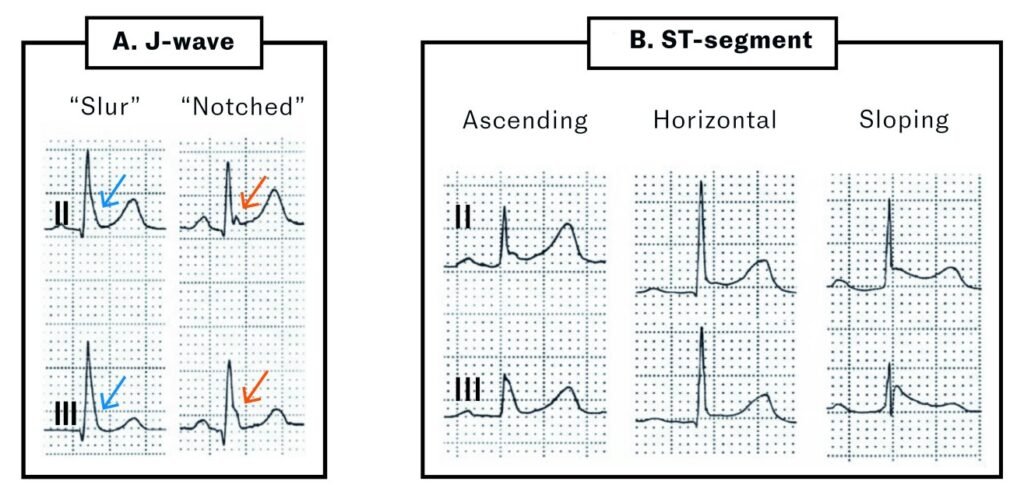
Different manifestations of early repolarization. Modified from Antzelevitch et al. A) The J wave may be well-defined (red arrow) or appear as a distortion of the terminal portion of the QRS complex, with the J wave ‘buried’ at the end of the complex (blue arrow). B) ST-segment elevation is common in early repolarization patterns but is not an absolute criterion. The ST segment may be ascending, horizontal or descending with the descending pattern more strongly being linked to arrhythmias.
Early repolarization syndrome and Brugada syndrome are both channelopathies and together are classified as J‑wave syndromes (1). In Brugada syndrome, prominent J waves are seen in the right precordial leads V1–V3, creating an apparent ST‑segment elevation in these leads. In ERS, J waves are typically found in the inferolateral leads.
ERS and Brugada syndrome share several clinical features; cardiac arrest often occurs at rest or during periods of heightened vagal tone and is frequently triggered by short‑coupled premature ventricular complexes (PVCs). In the period preceding cardiac arrest, J‑wave augmentation and frequent PVCs are commonly observed. Another ECG marker associated with increased arrhythmic risk in ERS is post‑extrasystolic J‑wave augmentation, which is present ECG #2 and shown in greater detail in the figure below.
Fig #3
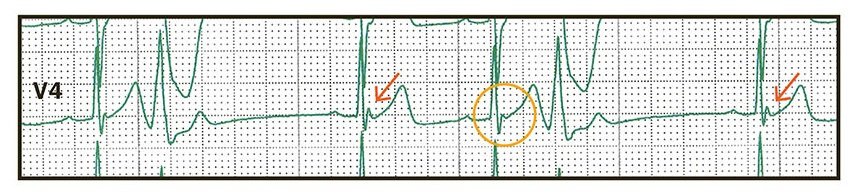
Rhythm strip from lead V4 immediately prior to cardiac arrest. QRS complexes preceded by a post-extrasystolic pause, and thus a prolonged RR interval, show more prominent J waves (arrows) compared with QRS complexes not preceded by RR interval prolongation (circle). This phenomenon is called post-extrasystolic J-wave augmentation and is a marker of arrhythmic risk in ERS (2).
The patient was treated with atrial pacing at 90bpm to prevent bradycardia and suppress premature ventricular complexes, which successfully averted further episodes of ventricular fibrillation. Unfortunately, the patient in this case had suffered a severe anoxic brain injury from the prehospital cardiac arrest and after prognostication it was ultimately decided to withdraw life support
Conclusion:
Should we be concerned about early repolarization and inform patients that their ECG pattern is linked to sudden cardiac death. The answer is no.
Early repolarization and J waves are extremely common findings. The incidence of ‘idiopathic’ ventricular fibrillation is very rare with an incidence of approximately 3 per 100,000 patient-years in individuals aged ≤45 years. For those with early repolarization, the incidence rises only modestly to 11 per 100,000 patient-years (3).
In other words, ERP is almost always an incidental finding without clinical consequences and J waves are almost always benign. It is only in very rare situations and certain contexts they may indicate an arrhythmic risk — this is particularly true when they are marked, accentuated and associated with bradycardia. This can occur in settings such as early repolarization syndrome (ERS), Brugada syndrome (BrS), or hypothermia.
Link to the full case report. A man in his 30s with cardiac arrest | Tidsskrift for Den norske legeforening
Learning points:
- ERP and J waves are extremely common. When present in isolation ERP is NOT a cause for further work up.
- ERS is a diagnosis of exclusion and should only be considered when other potential causes of ventricular fibrillation have been ruled out and an early repolarization pattern is documented on the ECG.
- ERS and BrS are clinically similar, characterized by J waves and associated with sudden cardiac death. Together ERS and BrS are referred to as the J‑wave syndromes.
- Management of ERS (and BrS) is centered on ICD implantation. Quinidine is the drug of choice in patients with a high arrhythmic burden.
References:
- Antzelevitch C, Yan GX, Ackerman MJ et al. J-Wave syndromes expert consensus conference report: Emerging concepts and gaps in knowledge. J Arrhythm 2016; 32: 315–39. [PubMed][CrossRef]
- Nam GB, Kim YH, Antzelevitch C. Augmentation of J waves and electrical storms in patients with early repolarization. N Engl J Med 2008; 358: 2078–9. [PubMed][CrossRef]
- Aagaard P, Sydow J, Börjesson M et al. Early repolarization in ECG. Definition, prevalence and prognostic significance. Lakartidningen 2015; 112: DLUT. [PubMed]
= = =
======================================
MY Comment, by KEN GRAUER, MD (2/5/2026 ):
Today’s unfortunate case reviews the events of an unwitnessed cardiac arrest that occurred in the home of the patient. Although initially resuscitated by emergency services — this previously healthy man in his 30s ultimately succumbed as a result of severe anoxic brain injury sustained from the prolonged delay until the patient was discovered.
- My Confession: As interesting and insightful as Dr. Nossen’s discussion is — it raises more questions for me than it answers. I find the subject of ERS (Early Repolarization Syndromes) not only utterly confusing — but further complicated by a need to distinguish the potentially lethal entity of ERS — from the similar-sounding but almost always benign entity of ERP (Early Repolarization Pattern).
= = =
To repeat the accepted definition of ERS (Early Repolarization Syndrome) that Dr. Nossen provides in his above discussion:
- ERS — is an arrhythmia syndrome in which the patient has ERP (Early Repolarization “Pattern”) on ECG and has had one or more malignant arrhythmias and/or an episode of sudden cardiac arrest.
- Critical to this definition of ERS — is the presence of ERP. But what is ERP?
= = =
What is ERP? (Early Repolarization Pattern)?
The concept of ER (Early Repolarization) used to be simple. No more …
- There used to be consensus among clinicians that ER ( = “early repolarization” ) was a common finding most often seen in otherwise healthy young adults (especially blacks) — in which there is mild ST elevation, sometimes in multiple leads — often associated with J-point notching — with a benign longterm prognosis (which is why this entity was called by many “BER” = Benign Early Repolarization).
- The primary clinical relevance of recognizing ER — used to be limited to distinguishing this common, benign ECG finding from acute pericarditis and acute infarction.
- This all changed in 2008 — when Haïssaguerre et al found an increased prevalence of ER in patients with idiopathic VFib (N Engl J Med 358:2016-2023, 2008). Since then — the challenge has been to try to distinguish between the very common ECG finding of early repolarization vs asymptomatic individuals with ERP who have a significant risk of developing a malignant arrhythmia.
- As I note and reference in My Comment at the bottom of the page in the May 23, 2022 post of Dr. Smith’s ECG Blog — the prevalence of ER in the general population has been cited to range between 2-to-31% — with this percentage depending on age, sex, race, differing terminology, and especially the amount of J-point elevation accepted as “qualifying” for the definition. This variance in the prevalence of ER by itself highlights the lack of consensus among clinicians for what does and does not constitute criteria for “Early Repolarization” (with this complicating the definition of “ERS” — since criteria for ERS are dependent on the presence of ERP).
- Macfarlane, Antzelevitch, Haissaguerre, Tikkanen, Wellens et al — in their 2015 Consensus Paper (JACC 66(4):470-477, 2015) — acknowledged this lack of agreement among clinicians for defining ERP — and these experts put forth their new definition of ERP:
- NOTE #1: For readers of this Blog wanting to clarify what these authors identify as a “notch” and/or “slur” — there are many helpful figures in this JACC paper. That said — the measurement parameters used to define these ECG findings are more complex than what I’d want to recommend to the busy, practicing clinician.
- NOTE #2: Despite my hours spent trying to sift through the ERP/ERS literature — I remain uncertain about whether there is any difference between use of the terms “ER“ (Early Repolarization) vs “ERP“ (Early Repolarization Pattern). I am therefore using these terms interchageably.
- NOTE #3: By the Macfarlane et al new definition — ST elevation is no longer required to satisfy criteria for “ERP”. All that is needed is “slurring” or “notching” meeting the specifications cited below.
= = =
Details of the Macfarlane et al 2015 definition of ERP:
- Early Repolarization (by the Macfarlane et al definition) — is said to be present on ECG if each of the following Criteria are met: i) There must be an end-QRS notch (J wave) or “slur” on the downslope of a prominent R wave — and this notch or “slur” must lie entirely above the baseline; — ii) The peak of this notch (Jp) must be ≥0.1 mV ( = 1mm) elevated above the baseline in ≥2 contiguous ECG leads (excluding leads V1-V3 — to avoid confusion with a Brugada pattern). IF there is a “slur” (instead of a notch) — the onset of the slur must be ≥0.1 mV ( = 1mm) elevated above the baseline; — and, iii) These ECG findings should be associated with prominent T waves (in ≥2 contiguous ECG leads) — and — a QRS duration (measured in leads that do not show a slur or a notch) that is less than 0.12 second in duration.
- ST segment elevation without notching or slurring (as specified by the above criteria) — should not be considered “ER” by the Consensus Paper authors. Instead — they state that the term nonspecific ST elevation should be used.
- ERP does not require ST elevation (by the newer definition).
= = =
A year later in 2016 — Patton headed a panel of 10 experts (all being different experts from the 10 experts on the 2015 Macfarlane panel) — in which Patton et al issued an AHA Scientific Statement emphasizing a different perspective (Circulation 133:1520-1529, 2016).
- Patton et al open their AHA Scientific Statement by acknowledging that although ERP began as a “benign entity in which ≥1 leads manifest ST elevation” — “more recent studies have demonstrated positive, negative and neutral associations between an ERP and various end points, including all-cause, cardiac and arrhythmic mortality” — with those studies using “more complex definitions of ER” including J-wave notching or slurring with or without ST elevation.
- Patton et al go on to say, “As a result — considerable confusion remains concerning the definition of ERP, its prognostic significance, and whether additional evaluation or treatment is warranted”.
- Patton et al conclude that many challenges remain for interpreting ERP in the clinical setting with “a lack of knowledge underlying the understanding of this very prevalent condition”.
= = =
Bottom Line: What I Think is Important to Remember
As per my synthesis from the above papers by Macfarlane et al and Patton et al — which I found summed up by Sayedahmad et al (Cleveland Clin J Med 86(30):165-166, 2019):
- Consensus is lacking among experts regarding how best to define ERP. This remains a source of confusion among practicing clinicians — which is especially important given the prevalence of ER in the general population.
- That said — the incidental detection of some form of a “repolarization variant” (be this by Macfarlane, Patton or other criteria for ER) on an otherwise normal ECG — obtained from an otherwise healthy individual in the absence of a worrisome arrhythmia, syncope/presyncope, or a positive family history for sudden death or malignant arrhythmia — is almost always a benign finding not in need of further evaluation.
- Not necessarily so when ERP is seen in a patient who does present with a worrisome arrhythmia (or a history thereof) — or with syncope/presyncope or a positive family history.
- And, an alarming finding in a patient with ERP who presents with a worrisome arrhythmia and/or syncope/presyncope — is the presence of J-waves in multiple leads, especially when serial tracings show J wave augmentation (as was seen in today’s case).
= = =
P.S.: Worthy of mention in the above cited reference by Sayedahmad et al — is the proposed mechanism for ERP that is associated with “notching” or “slurring”:
- The presence of J-wave notching or slurring may reflect an ion imbalance that results in a dispersion of refractoriness in multiple myocardial regions displaying variable levels of myocardial excitability.
- This may produce a voltage gradient between different myocardial areas — with unpredictable levels of myocardial excitability (which is manifested on ECG by notching and/or slurring — with “augmentation” of these findings on serial ECGs reflecting increased instability and arrhythmic risk).
- As Was Seen in Today’s CASE: Be aware of J waves that are seen in association with patients who present with a worrisome arrhythmia (as in ECG #1) and/or with syncope/presyncope or a positive family history — especially when there is J wave notching (or slurring) showing augmentation on serial tracings (as in Fig. #3).
= = =
= = =