Written by Pendell Meyers
A man in his 50s with HTN, HLD, obesity, and restrictive lung disease presented with shortness of breath worsening over the past 3 days. He also had a cough and subjective fevers. He denied chest pain. His vitals were within normal limits.
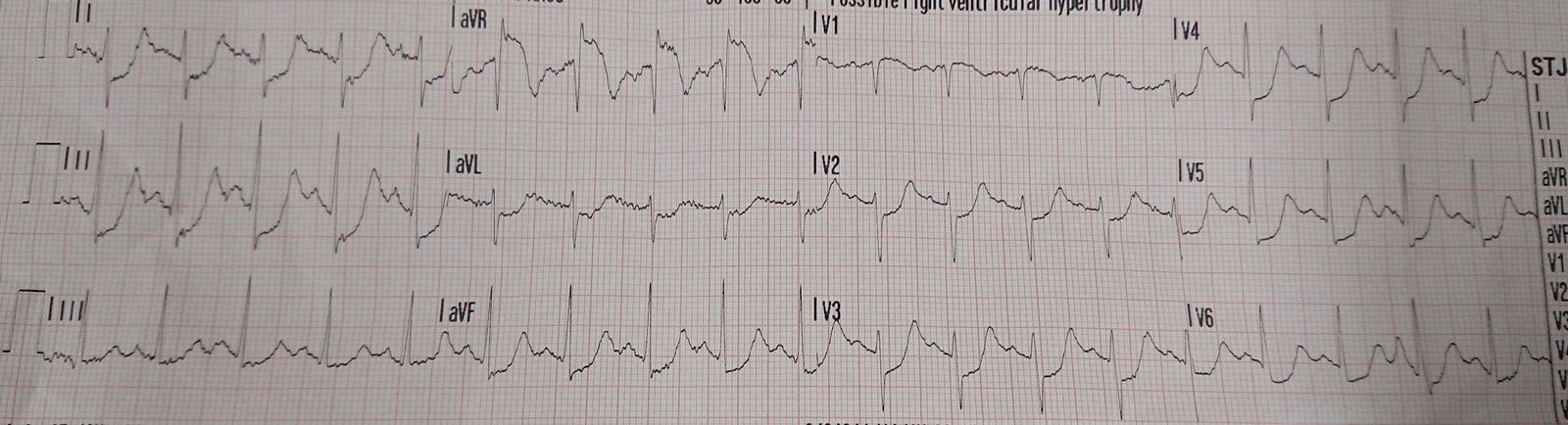
Here is his triage ECG (no baseline available):
 |
| What do you think? |
Findings:
– sinus rhythm at about 100 bpm
– STE in I and aVL (meets STEMI criteria)
– hint of STD in III and aVF
– STD in V1 and V2
– hyperacute T-waves in I and aVL (with reciprocal negative hyperacute T in III)
Interpretation:
This is definitive evidence of acute transmural injuryand active infarction of the lateral and posterior walls. In any adult population with symptoms potentially compatible with ACS, the most common etiology of this focal transmural ischemia is Occlusion MI (type 1 ACS). But there are other etiologies such as coronary spasm, takotsubo/stress cardiomyopathy (which rarely has reciprocal findings because it is usually widespread), focal myocarditis (rare, but usually does have reciprocal findings), etc. The cells of the posterior and lateral walls do not know the etiology of the transmural injury, and the ECG findings are the same regardless of the etiology.
Back to the Case:
With his infectious and respiratory symptoms and complete lack of chest pain, we did not activate the cath lab despite the ECG meeting STEMI criteria. Instead, we called cardiology to assist us in the ED to make sure that they agree he does not need emergent catheterization. We performed a bedside (non-contrasted) cardiac ultrasound together which showed globally decreased EF, and we were unable to appreciate a discrete wall motion abnormality in the posterior or lateral walls (very limited to due point of care and lack of contrast). If there is no wall motion abnormality on very high quality contrast-enhanced echo, it is unlikely that the ECG findings represent acute OMI.
Ultimately cardiology decided not to proceed with cath lab activation due to a combination of lowered clinical suspicion of ACS given lack of chest pain and presence of more infectious symptoms, as well as preliminary ultrasound findings. However, I think it would also have been perfectly reasonable to cath him regardless to definitively rule out ACS as the cause, because the harms of a diagnostic cath without intervention are minimal compared to the harm of untreated OMI.
The first troponin T resulted at 1.34 ng/mL (quite elevated), and subsequent measurements were 1.29 and 1.27 ng/mL.
Formal echo confirmed diffuse hypokinesis with severely depressed systolic function, EF 25%. No contrast was used, but there was no focal wall motion abnormality seen.
Covid PCR resulted positive.
CXR also revealed bilateral opacities consistent with covid pneumonia.
No cath was performed.
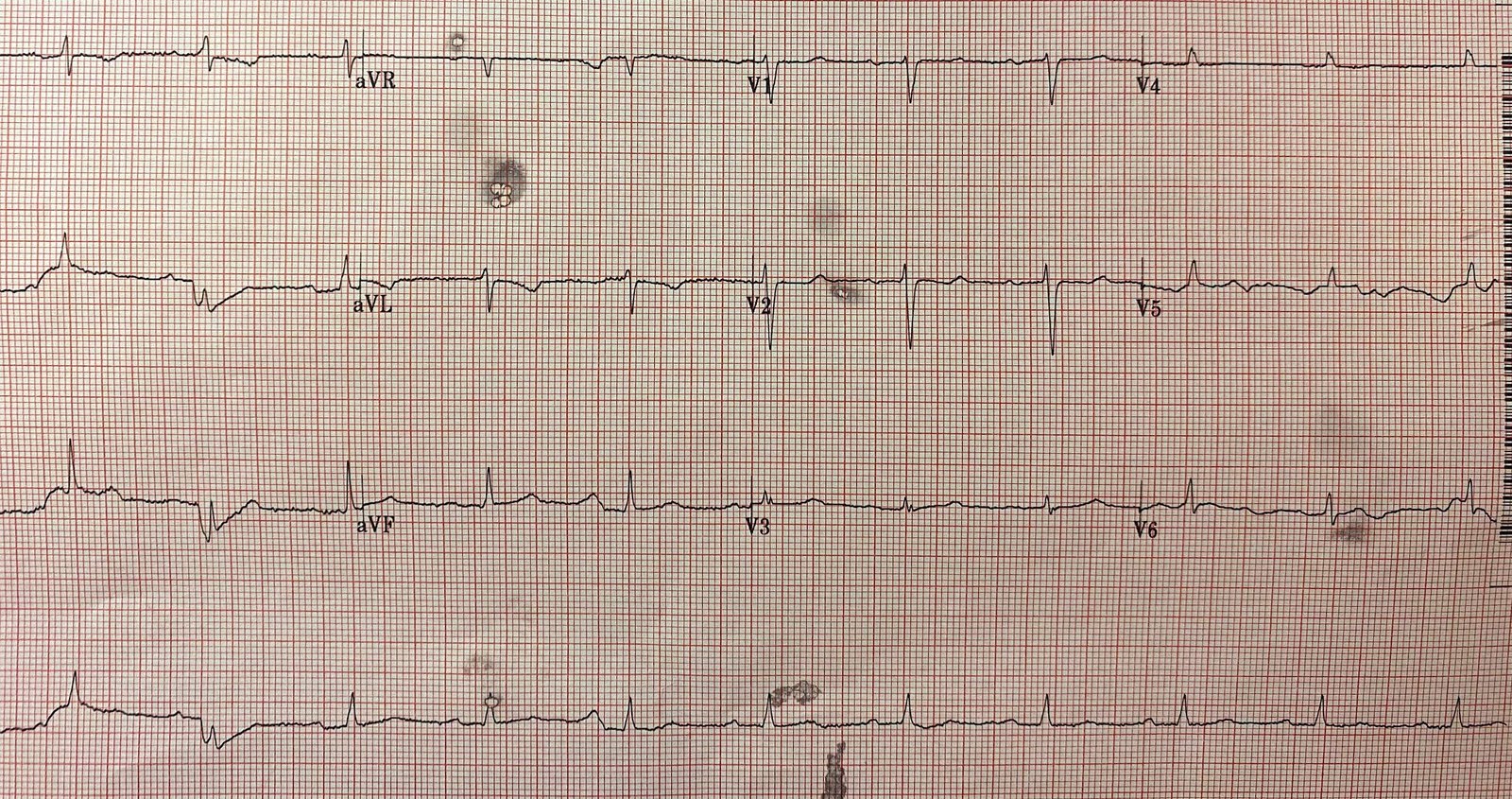
A repeat ECG was done several days later:
 |
| Poor quality. Focal lateral findings are much less pronounced, but still slightly present. |
The patient had an otherwise uneventful course and was discharged home with follow up to evaluate his long term cardiac function.
Learning Points:
COVID may cause myocarditis. However, myocarditis is not definitively proven in this case. If a high quality echo with contrast had shown no focal wall motion abnormality during ECG findings, then we could be almost assured that this case was definitively myocarditis. Short of that, myocarditis is only certain with biopsy or MRI (both of which were not performed in this case). It is still possible that this patient had true Occlusion MI (and STEMI), and he also happened to have COVID.
Myocarditis can be focal, and can be completely indistinguishable from OMI on ECG. Although the clinical picture is vitally important, clinical features alone are not enough to definitively distinguish focal myocarditis from OMI.
The decision to avoid emergent cath lab activation in a patient with shortness of breath, highly elevated troponin, and OMI findings on ECG (even STEMI[+] in this case) should not be made lightly. It may arguably be the right thing to do on a population level to perform the cath even knowing there is a high chance of a false positive, because the harms of one missed OMI are likely far greater than the harms of many false positive diagnostic caths without intervention.
![]()
===================================
MY Comment by KEN GRAUER, MD (5/11/2020):
===================================
Given the prevalence of Covid-19 infection — this case by Dr. Meyers is extremely relevant. It provides a superb illustration of clinical decision-making, in which despite ECG findings consistent with acute STEMI — the decision was made (wisely) not to proceed to cardiac catheterization.
- Presumably (although not definitively proven) — the patient in this case had acute myocarditis.
- To re-emphasize the key LEARNING Point highlighted by Dr. Meyers — Acute myocarditis can be focal, and can at times be completely indistinguishable from acute OMI on ECG. Consideration of clinical features may help in distinguishing between these 2 entities — but even then, a definite diagnosis cannot always be made. When doubt persists — prompt cardiac cath may be needed to exclude the possibility of acute OMI.
I have little to add to the excellent clinical discussion by Dr. Meyers. I limit my comments to a few additional “picky” points I’d add regarding ECG interpretation of the 2 tracings shown in this case (Figure-1):
- As per Dr. Meyers — ECG #1 shows sinus rhythm at a rate just under 100/minute. All intervals are normal. I would describe the frontal plane AXIS as indeterminate — as all 6 limb leads are close to being isoelectric.
- PEARL #1 — Determination of frontal plane axis is usually easy — and with experience, can usually be accomplished within seconds. That said — IF ever you find it taking you more than 2-3 seconds to figure out the frontal plane axis — chances are that the axis is indeterminate! That’s the case here. Looking at lead I in ECG #1 — one might think the axis is rightward. But looking at the 3 inferior leads — one might think there is LAHB. The reason for this discrepancy is that the axis lies in “No-Person’s Land” (ie, in the upper right quadrant). (NOTE: For those wanting a quick primer on Axis determination & the Hemiblocks — CLICK HERE. If you’d like a Video Review on Axis & the Hemiblocks — CLICK HERE).
- PEARL #2 — It’s helpful to keep in mind the 3 most common Causes of an Indeterminate Axis. These are: i) RVH; ii) Chronic pulmonary disease; and/or, iii) Large body habitus. Clinically, in this case — we are told that this patient is obese and has restrictive lung disease.
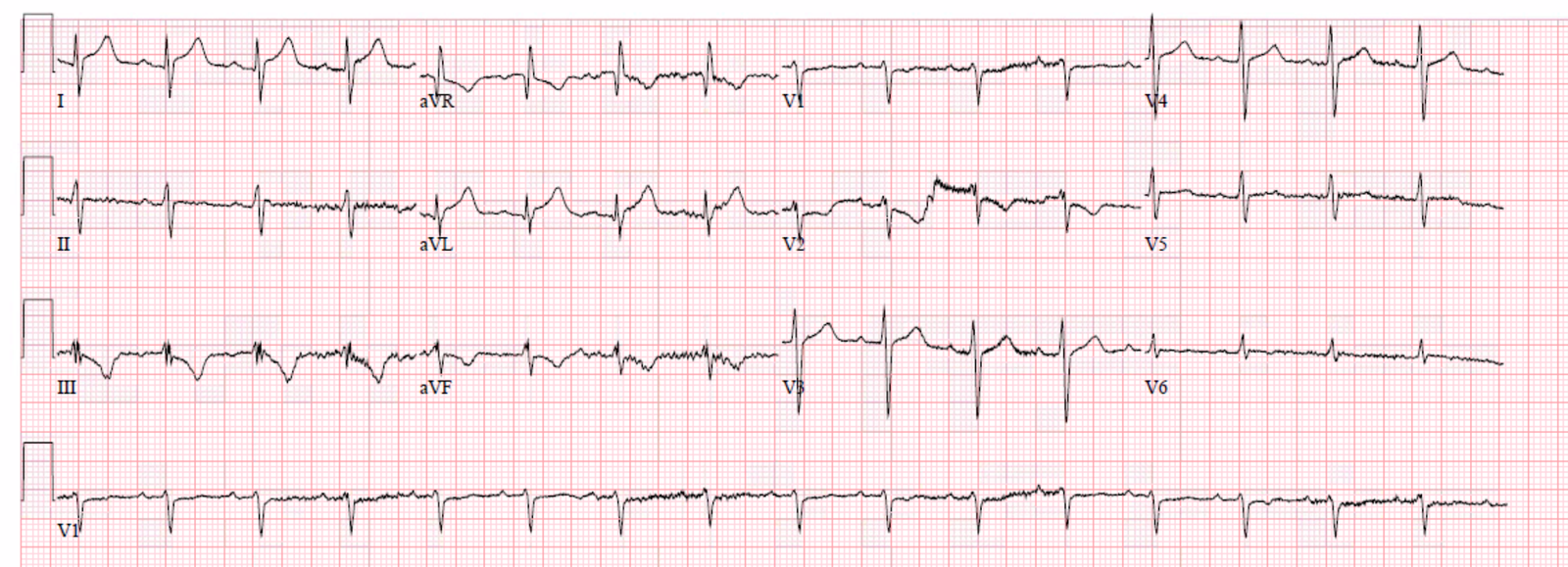
 |
| Figure-1: The 2 ECGs in this case (See text). |
Continuing with our Descriptive Analysis of ECG #1:
- Chamber Enlargement — None. Although the frontal plane axis is indeterminate — the rest of the ECG is not particularly suggestive of RVH. There is no sign of atrial abnormality or LVH.
- Q-R-S-T Changes — As per Dr. Meyers, there is ST elevation with hyperacute T waves in high-lateral leads I and aVL — with reciprocal (mirror-image) ST depression in leads III and aVF. There is also J-point ST depression in leads V1 and V2 (as per Dr. Meyers) — with an ST-T wave shape in lead V2 consistent with acute posterior involvement.
- WHY do you think the QRS complex in lead V6 of ECG #1 is so tiny? I’d surmise this may be due to either the patient’s obesity and/or his chronic pulmonary disease. The T wave flattening we see in leads V5, V6 is not a normal finding (Normally the T wave should be positive and of reasonable amplitude in leads V5,V6). I was not initially sure whether the flat ST-T waves in leads V5, V6 were a reflection of acute ischemia, the patient’s large body habitus, his chronic pulmonary disease — or some combination of these features.
- Clinical IMPRESSION of ECG #1 — As per Dr. Meyers, the above ECG findings could certainly be consistent with acute postero-lateral OMI. Alternatively (given the lack of chest pain, worsening dyspnea with positive Covid-19 assay) — the findings more likely represented focal acute myocarditis.
My THOUGHTS on ECG #2: This 2nd ECG tracing was obtained several days later. The patient had clinically improved — and was soon to be discharged from the hospital. As per Dr. Meyers — “focal lateral findings were much less pronounced, but still slightly present”. That said — WHAT makes it difficult to compare the chest leads in these 2 tracings?
- PEARL #3 — In my experience, the most time-efficient way to compare serial ECGs is to: i) First choose 1 of the tracings — and interpret this first tracing in its entirety (as we did above for ECG #1); THEN; ii) Compare the 2nd ECG with the 1st one — by looking lead-by-lead to see if there are any changes between the 2 tracings in lead I — in lead II — in lead III — and in each of the other 9 leads. The reason performing this lead-by-lead comparison is important — is that otherwise, you might MISS the fact that QRS morphology of lead V2 is so different in ECG #1 compared to ECG #2! Given this patient’s large body habitus — the most likely reason for this marked difference in QRS morphology in lead V2 between the 2 tracings is lead misplacement of this chest lead on one of the tracings. On occasion, this technical mishap can be very important to recognize — because trying to compare the ST-T wave changes we saw in ECG #1, with what we now see for the ST-T wave in ECG #2 — is like trying to compare “apples with oranges” (given how very different the QRS complex in lead V2 is in these 2 tracings …).
- Clinical IMPRESSION of ECG #2 Compared to ECG #1 — Both tracings show sinus rhythm at a rate ~100/minute. There’s more artifact in ECG #2. I’d once again interpret the frontal plane axis of ECG #2 as indeterminate. I agree entirely with Dr. Meyers — that the hyperacute high lateral and reciprocal inferior lead changes are far less pronounced than they were in ECG #1. And although there almost certainly is some difference in chest lead electrode placement between the 2 tracings — the overall ST-T wave appearance in the chest leads of ECG #2 looks benign.
Our THANKS to Dr. Meyers for presenting some important clinical considerations for ECG interpretation during the current Covid-19 pandemic.
![]()