A middle-aged male with several comorbidities including DM presented with chest pain. It had been on and off all day, then constant for 2.5 hours. It was central without radiation, sharp but also tight, and was 9/10. There was some cough, but no SOB; he reports COPD and has been using his inhalers without improvement. He also reports diaphoresis and tingling of his hands since the worsening of pain at 1700.
His BP was 160/90.
He was given aspirin and nitro via EMS with good improvement in his chest pain.
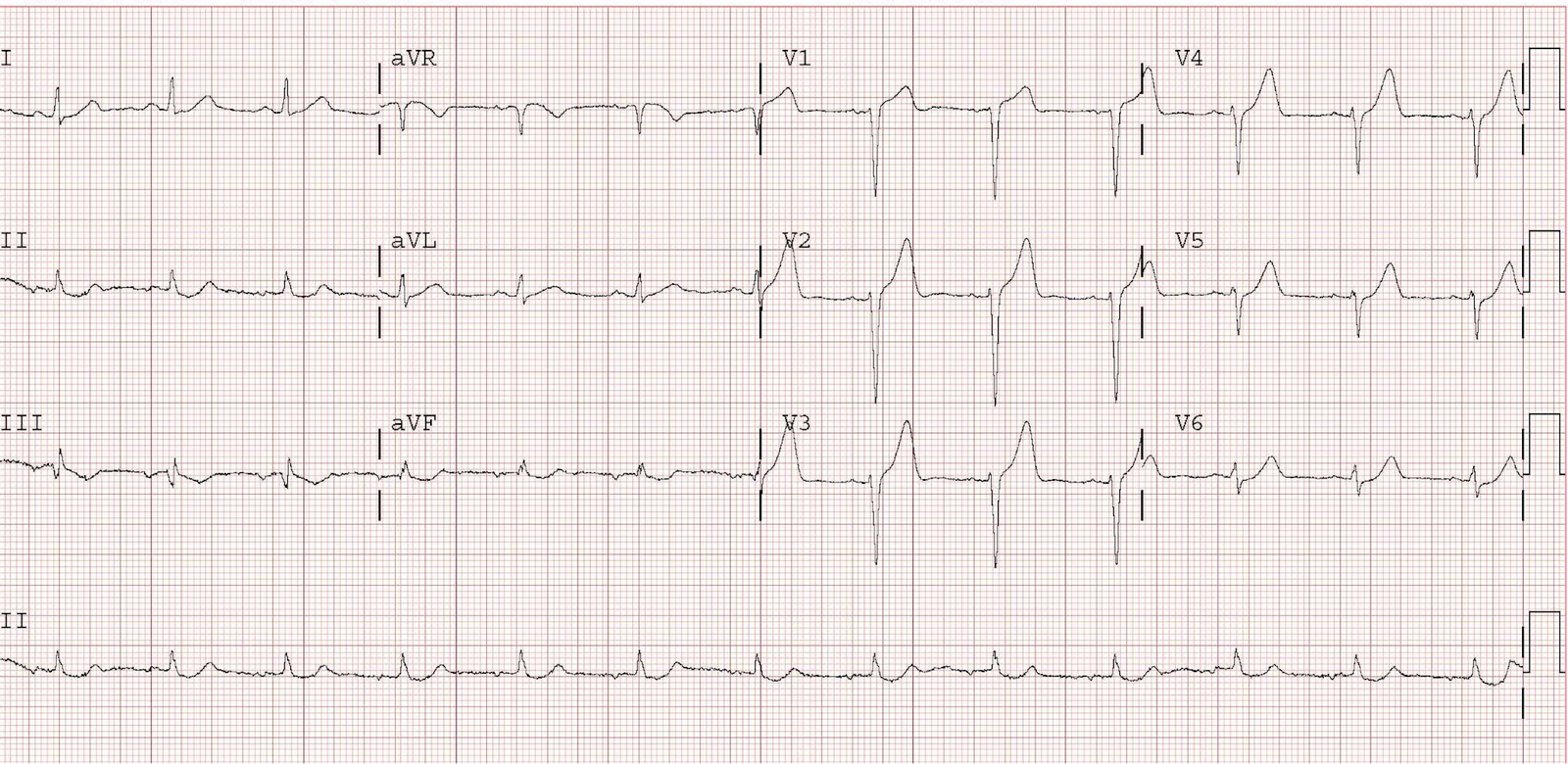
First ED ECG at 2:40 after chest pain became severe.
 |
| Sinus rhythm.
Slight left axis deviation (mostly negative QRS in II, R-wave aVL; axis about -40) There is a bit of suspicious flattening of the ST segment in inferior leads and a tiny bit of STE in aVL, but it is really non-diagnostic and nearly normal. |
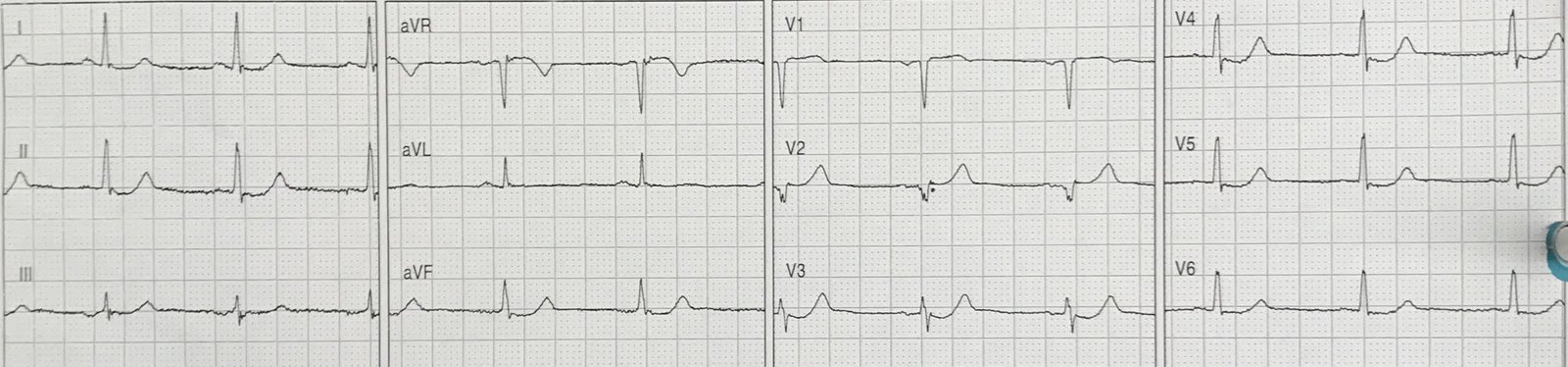
Here was a previous ECG while dehydrated a few months prior:
 |
| Sinus tachycardia.
In this ECG, there is a hint of ST elevation in III, with reciprocal ST depression in aVL. None of this was ischemic, but it does suggest the patient’s baseline is different from the presentation ECG above. |
Here I put limb leads one after the other for more close inspection:
II,III,aVF,aVL only: Presentation ECG

II,III,aVF,aVL only: Previous ECG

At approximately 30 minutes after arrival, the first troponin returned at 0.046 ng/mL (99% URL = 0.030 ng/mL)
The patient was put on heparin and Nitroglycerin, but his pain could not be controlled.
Another ECG was recorded:
 |
| There is lead reversal of limb leads.
As for the precordial leads, there is not much change. |
A bedside echo was performed:
The segment on the upper left is not contracting. This is the anteroseptal wall.
Here is a 4-chamber view:
The apex is not contracting.
From all this data, one should concluded that there is a coronary occlusion that is not showing on the ECG, until proven otherwise.
25% of acute coronary occlusion does not have diagnostic ST elevation. Many of those cases have ECG that are highly suggestive of ischemia. An unknown number of acute occlusions have normal, or near normal ECGs, but it is NOT uncommon, and one should be on the lookout for them.
A positive troponin in this clinical situation [no reason for an elevated troponin: no end stage renal disease, no heart failure, no reason for a type II MI (BP of 160/90 should not be thought to be a cause)], ALONG with the inability to control the pain with medical therapy is an indication for immediate angiography, according to the guidelines of both the American Heart/American College of Cardiology and the European Society of Cardiology.
This patient, based on just the 1) troponin and 2) refractory pain, should go emergently to the cath lab even with a normal ECG.
Actually, although he was put on IV NTG, it was not maximal. This should be titrated to a significant drop in BP, down to perhaps 110-120 systolic. This was not done.
The echo is just extra data to support that plan.
However, the vast majority of patients with NonSTEMI that really need the cath lab now do not go in a timely way. In fact, in this large meta-analysis by Khan et al. of 40,000 NonSTEMIs published in the European Heart Journal in August 2017, 25% had occlusion and it took 24 hours to get to angiography.
Unfortunately, this patient proved the rule rather than the exception. He was admitted with a diagnosis of NonSTEMI without immediate angiography.
But Fortunately, he was admitted to excellent internal medicine residents, who immediately recorded another ECG when he arrived upstairs.
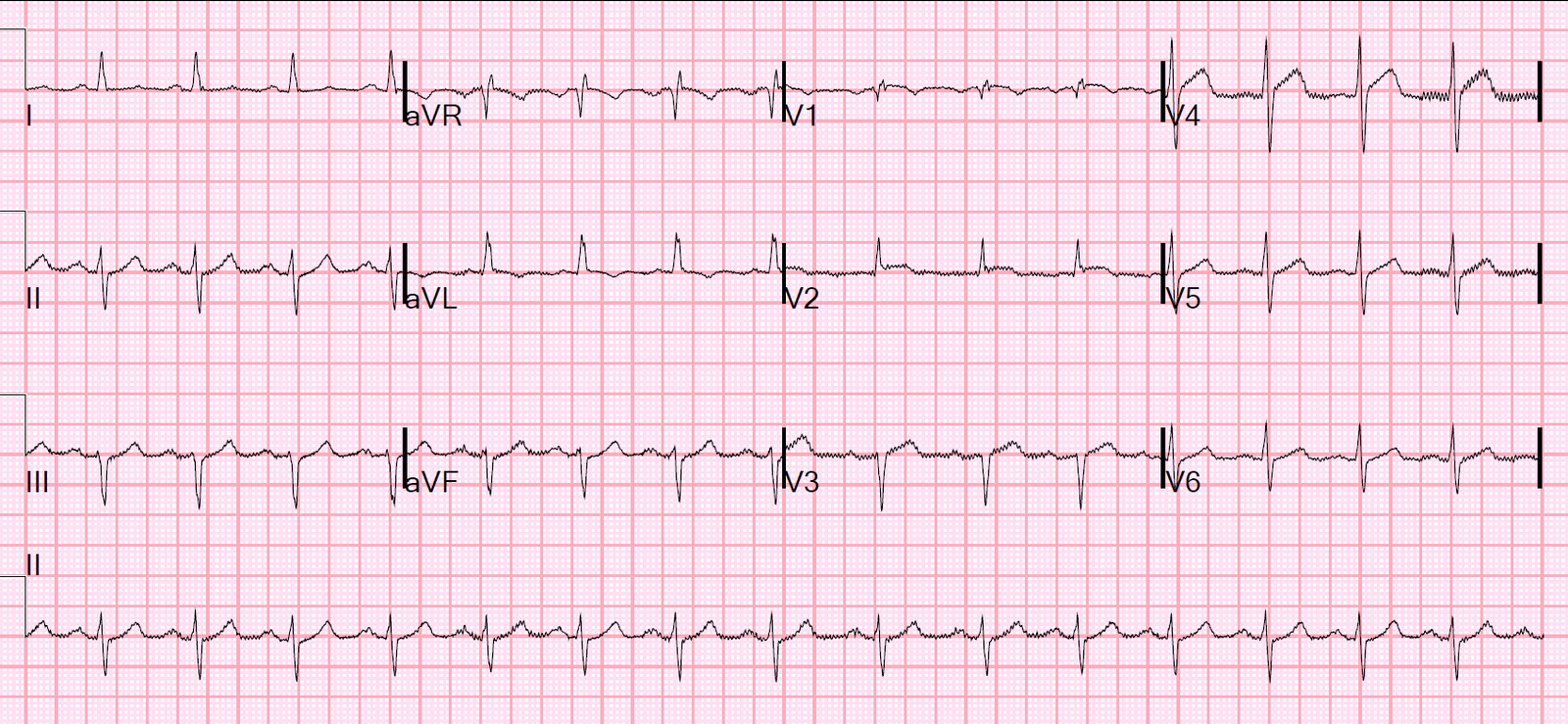
Here it is, one hour later:
 |
| Now there is diagnostic ST Elevation |
The cath lab was activated.
This was recorded just before angiography:
Angiogram:
Left ventricular descending coronary artery: 100% thrombotic occlusion in the midportion of the vessel distal to the origin of the first diagonal.
Next Day
 |
| Deep QS-wave in V3 |
Troponin profile

This was a big myocardial infarction!
Learning points:
1. Some coronary occlusion do not show on the ECG, or show only minimally.
2. Even serial ECGs may not show the MI
3. If the troponin is elevated in a patient with a chief complaint of chest pain, it is a type I MI until proven otherwise.
4. In a type I MI, if the symptoms can’t be controlled with antiplatelet, antithrombotic, and anti-ischemic therapy (NTG), then immediate cath lab activation is indicated.
5. Read your cardiac ultrasounds carefully. Wall motion abnormalities are hard to see. You can only say there is no wall motion abnormality if: 1) The images are very high quality, with bubble contrast, and 2) you are expert.