I received this case from a medic (in quotes):
“Wanted to know your thoughts on this ECG.”
“Woman in early 70’s with acute chest pain for the past 30 min. Vomited once. Looked sick. Pale and diaphoretic. Had hx of MI with stents one month ago. No old ECG to compare with. I interpreted the ECG as a LBBB with sinus tach but some thought it was VT. We administered Aspirin and transported to hospital.”
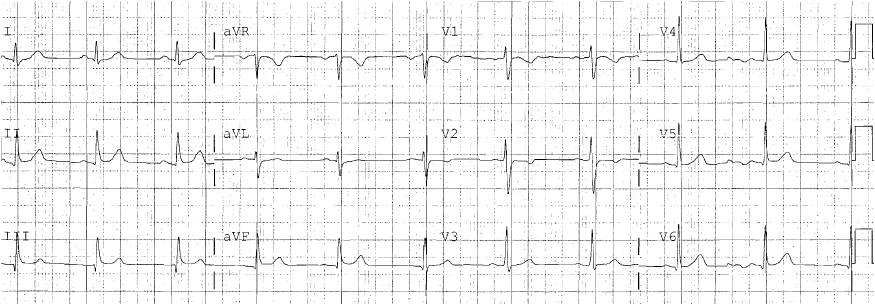
Here is the prehospital ECG and the only one he sent:

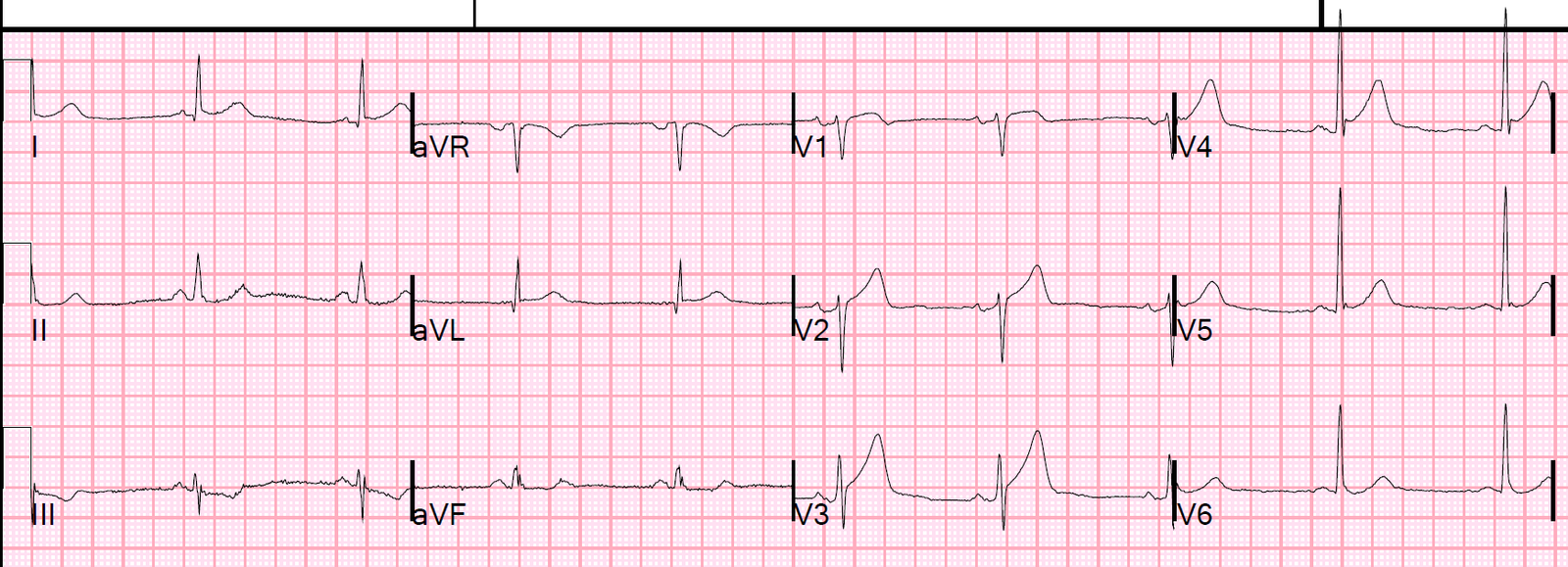
| Smith comments: There are clear P-waves (see arrows in image below) with a regular rhythm. The computer interpretation is clearly wrong; it is clearly sinus tachycardia. However, it does fairly accurately measure ST elevation at the J-point (this was printed out on the tracing!) Notice there is LBBB. There is subtle concordant ST elevation in leads I and aVL. There is at least 2mm (I doubt 3.03) of STE in V3, with a 6 mm S-wave, for a ratio of 0.33 There is 1 mm of STE in V4 with a 1 mm S-wave, for a ratio of 1.0 It meets modified Sgarbossa in several leads It is diagnostic of a proximal LAD occlusion in the setting of LBBB |
Same ECG, annotated with arrows
 |
| See clear P-waves (arrows). In V1, the P-waves are negative, as they should be (the later portion of the P-wave represents the left atrium and is normally negative). This helps to verify they are P-waves. |
Comment
Whenever there is sinus tachycardia, one must consider whether the tachycardia is secondary to some other acute pathology (GI bleed? Pulmonary embolism? Ruptured AAA? Sepsis? etc.), and the ST elevation is due to the tachycardia and to this other illness (supply demand mismatch with demand ischemia and type II MI). But this patient has a clear history of chest pain onset. It is very typical of STEMI with acute cardiogenic shock.
Case continued:
“Upon arrival, she went into V Tach with a pulse and was cardioverted by attending and then coded. She was intubated and resuscitated.”
“What are your thoughts? LBBB vs V Tach? Any signs of potential MI?”
My answers are above.
Outcome
“The medic tried to communicate his concerns to ED attending but was told it did not meet STEMI criteria. Patient arrested in ED and was resuscitated, intubated and admitted to ICU. They did not take her to the cath lab. The next day troponin came back positive (not sure what value was) and like you said patient was in cardioogenic shock with severe acidosis and renal failure. She arrested again in ICU and could not be resuscitated.”
Learning Points:
1. Even had the ECG not been diagnostic, the history is classic for ACS with cardiogenic shock. This is an unequivocal indication for emergent reperfusion therapy
2. This ECG is diagnostic of STEMI in the setting of LBBB. It should erase any doubt about the etiology of shock
3. Listen to the medics!