
A young man had sudden syncope without a prodrome, after which he was aysmptomatic. He presented to an ED and had this ECG recorded:
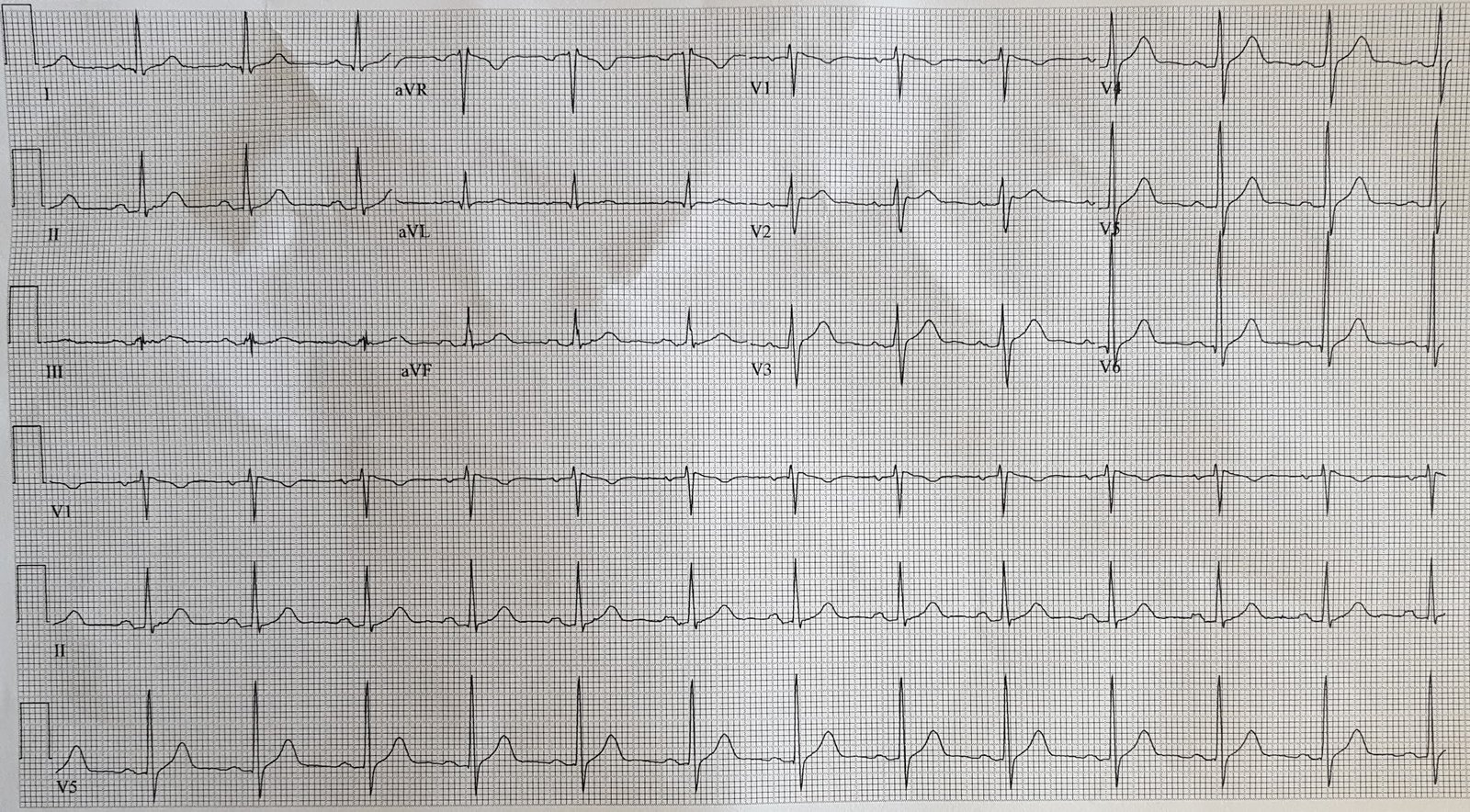 |
| What do you see? |
There is an abnormal rSr’ in V1, with the r’-wave not falling quickly back to baseline. The T-wave is inverted, but this is also a normal finding in V1. The whole morphology is suggestive of Brugada morphology, but by no means “diagnostic” because the r’-wave is not 2 mm.
Here are the criteria for ECG Brugada morphology. This comes from the paper entitled (with full text link): Current electrocardiographic criteria for diagnosis of Brugada pattern: a consensus report
Criteria for Type 1 Morphology:
1. R’-wave at least 2 mm in V1 or V2
2. But no distinct R’-wave because the ST segment takes off at an angle from the peak
3. The ST segment is convex upward (“coved”). [They use terminology of “concave downward”]
4. The peak at the high takeoff does not correspond with the J-point. It is BEFORE the J-point, as measured in other leads (such as lead II across the bottom).
5. Gradual downsloping of ST segment such that at 40 ms after the takeoff, the decrease in amplitude is less than 4 mm. In normal RBBB, the decrease in amplitude is much greater (see this example).
6. ST is followed by a symmetrically negative T-wave
7. “The duration of QRS is longer than in RBBB,” and “there is a mismatch between V1 and V6.” This criterion is perplexing and not well explained.
8. The downsloping should be such that the Corrado index is greater than 1.0.
This is the ratio: [ST elevation at the J-point] divided by [ST elevation at 80 ms after the J-point].
Diagnosis of Brugada Syndrome requires both:
1. Brugada pattern ECG (either Brugada Type 1, or the newly defined Brugada Type 2)
Findings may be dynamic and are sometimes concealed; findings may be observed only in certain circumstances such as fever, intoxication, electrolyte imbalance, presence of sodium channel medications/drugs, or vagal stimulation.
2. At least one of the following:
(a) survivor of cardiac arrest,
(b) witnessed/recorded polymorphic ventricular tachycardia (VT),
(c) history of nonvagal syncope,
(d) familial antecedents of sudden death in patients younger than 45 years without acute coronary
syndrome
(e) Type 1 Brugada pattern in relatives.
Criteria for Type 2 Brugada morphology:
First, there must be:
a) An RSr’ with a typical saddleback pattern in V1 and/or V2.
b) V1 may have either an upright, flat, or inverted T-wave (in our case above it is inverted).
c) T-wave in V2 is usually but not always positive.
d) Minimum ST segment ascent of 0.5 mm. There could be no saddle without an ascent.
Once these are fulfilled, there should be, in lead V2:
1. High take-off of the descending limb of the r’ at least 2 mm above the isoelectric line (in our case, it is less than 2 mm, so this does not meet criteria for Type 2 Brugada). The r’-wave is thus not distinct, as it is in benign causes of rSr’
2. Mismatch between QRS duration in leads V1 and V6 (longer in lead V1). This helps to distinguish from RBBB, in which the QRS duration is equal in V1 and V6.
3. As with Type 1, the peak of the r’-wave does not correspond to the J-point in other leads.
4. A large Beta angle. Go to this post to learn about the beta angle.
So this ECG cannot be said to fulfill the criteria for either type 1 or type 2 Brugada, but it is suggestive, and the patient had non-vagal syncope.
Case continued:
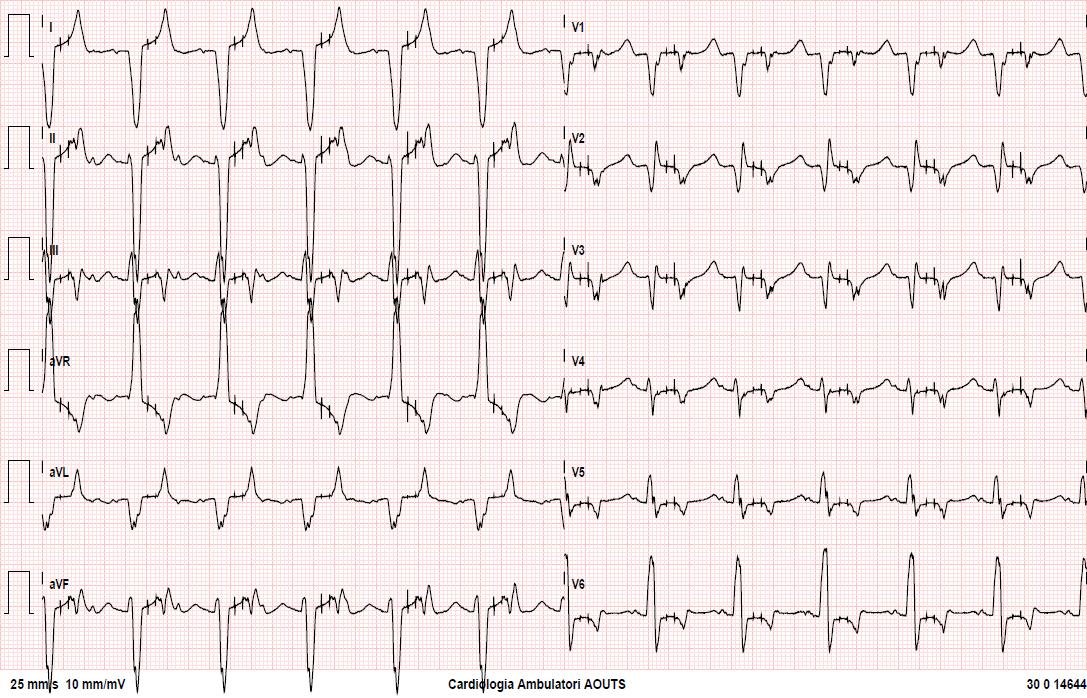
The patient presented with syncope and fever 3 years later. Here is the ECG:
 |
| Now the ECG, in the presence of fever, is diagnostic of Brugada morphology |
The patient underwent an EP study and had a ICD implanted.
Learning Point:
The patient and doctor dodged a bullet here. He could have died in the intervening 3 years. This sort of cardiac syncope is death that terminates with awakening.
The first ECG is nonspecific but suggestive of Brugada, and in the context of non-vagal syncope the patient should at least get early referral to a cardiologist, preferably an electrophysiologist, for EP testing or for challenge with a sodium channel blocker.
Read more about Type 1 and Type 2 Brugada syndrome here:
Is this Type 2 Brugada syndrome/ECG pattern?
Here are many articles on Fever unmasking Brugada syndrome:
https://scholar.google.com/scholar?hl=en&q=brugada+fever&btnG=&as_sdt=1%2C24&as_sdtp=
{kind=link}