An 80-something tripped and sustained a hip fracture.
The patient had no cardiac symptoms, no syncope, no CP or SOB. He was perfectly fine.
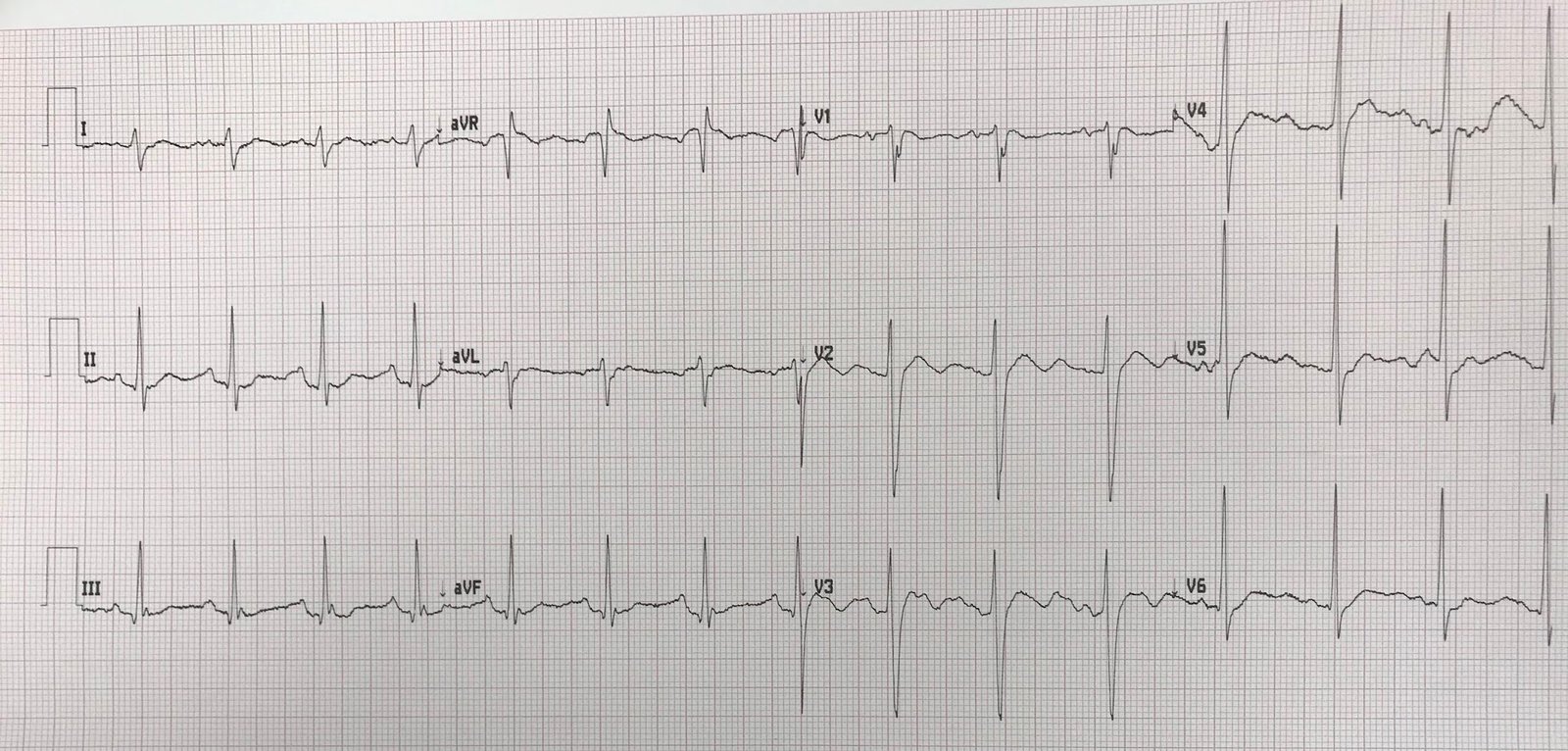
He had a 12-lead ECG in the ED as part of screening:
 |
| Interpretation? |
You know there is something wrong at least partly because it is on this blog.
But this was looked at in a cursory fashion by a couple very busy emergency physicians and no serious abnormality was noticed.
First note that the QRS complexes are grouped. Then you can see that there are P-waves which did not conduct (#’s 3 and 8). There is no PR lengthening prior to the blocked conduction; therefore, it is not Mobitz I (Wenckebach), which would be a benign AV block, but rather Mobitz II.
They did not see that this is 2nd degree AV block Mobitz II. When I saw it I immediately recognized it, after which it was clear to the providers.
Mobitz II has dropped beats without any prior PR lengthening, and is at risk of progressing to 3rd degree (complete) AV block. Mobitz II is often below the AV node and therefore often does not respond to atropine. When the QRS is wide, then it is much more likely to represent blockade below the AV node, and is more likely to be dangerous.
In this case, there is also RBBB with LAFB, which suggests block below the bundle of His.
Clinical Course
Pacer pads were placed on his chest and he was admitted to the ICU with cardiology and EP consultation.
Had he had this rhythm associated with symptoms such as syncope, or associated with acute MI, then he would undergo immediate transvenous pacer placement.
He was kept overnight on telemetry and on the cardiac monitor he was noted to have intermittent bradycardia. Some of them were during sleep hours, however there was another episode around 10 PM where it is not very clear whether he was asleep or not.
Of note, the PR interval is normal during the conducted beats. This is important because it suggests that vagal tone did not have anything to do with the AV block, and suggests a more pernicious etiology.
There was concern that, during hip surgery, he would develop complete AV block.
A temporary pacer was placed.
An EP study to assess need for permanent pacer was undertaken and showed no convincing evidence of Infra-His block. No permanent pacer was placed.
Learning Point:
Assess the ECG systematically or you will miss something, especially when it is a screening ECG (i. e., the patient does not have cardiac symptoms)!
These are the characteristics of a normal ECG.
Note that you must assess the rate, rhythm, P-waves, PR interval, and a QRS for every P-wave as part of a systematic approach.
NSR,
normal rate
Upright
P wave in lead II
Biphasic P wave in V1
PR
interval 120 – 200 msec
QRSforeveryP-wave,samePRinterval
QRS less than 110 msec
Normal QRS Axis (-30 to 90 degrees)
Voltage
normal
Normal
septal Q waves
Normal
R-wave progression
Normal
ST segments
Normal T-wave size
Normal
T wave axis
Normal
QT
Normal
U-waves
![]()
===================================
MY Comment by KEN GRAUER, MD (1/1/2020):
===================================
I like nothing better than a good arrhythmia to start of the new decade! So our THANKS to Dr. Smith for doing just that. I’d add the following thoughts to the excellent discussion by Dr. Smith.
- As per Dr. Smith — perhaps the KEY Learning Point is the need to use a Systematic Approach to ECG Interpretation (and especially to rhythm interpretation). Readers of Dr. Smith’s blog know I constantly emphasize this point (See My Comment in the June 28, 2019 post on Dr. Smith’s blog).
- CLICK HERE — For “My Take” on Systematic 12-Lead interpretation.
- CLICK HERE — For “My Take” on Systematic Rhythm interpretation.
Regarding this 12-lead ECG + Rhythm Strip:
- As per Dr. Smith — There is underlying RBBB/LAHB — but there are no acute changes.
- Regarding the rhythm — we look first at the long lead rhythm strip. The underlying rhythm is sinus (ie, upright P wave in lead II) — with slight sinus arrhythmia (slight variation in the R-R interval).
- The QRS complex is wide (as above = RBBB/LAHB).
- The overall R-R interval is fairly regular — but there are 2 pauses on this lead II rhythm strip.
- As per Dr. Smith — the PR interval remains constant for the conducted beats throughout this rhythm strip! PEARL #1 — The KEY to diagnosing Mobitz II, 2nd-Degree AV Block — is that you see consecutively conducted beats, in which the PR interval does not increase. The reason you cannot distinguish with certainty between Mobitz I vs Mobitz II forms of 2nd-Degree AV Block when there is strict 2:1 AV conduction — is that you never get to see 2 conducted beats in a row when there is 2:1 AV block (which means that you can not tell for sure if the PR interval would increase [as in Mobitz I ] IF it had a chance to do so).
- The patient in this case was in his 80s. We have no idea for how long he has lived with bifascicular block + Mobitz II. This AV block could be recent or acute (therefore the rationale for placement of a temporary pacemaker) — but given the subsequent negative EP study — the thought was that permanent pacing was probably not necessary at this point in time (and might never be necessary for this patient in his 80s).
- That said — this potentially serious (life-threatening) form of AV block should not have been overlooked by the initial providers. PEARL #2 — IF emergency providers would begin to routinely carry and use a pair of Calipers — they will doubtlessly surprise themselves by increasing their speed for interpreting complex arrhythmias — and, I bet they will never again miss another case of AV block!
- PEARL #3 — Assuming this 80-something patient maintains his satisfactorily functional lifestyle status — I would recheck a 24-hour Holter monitor on him fairly soon (and perhaps periodically as an outpatient in the future) — to ensure that prolonged bradycardia does not subsequently develop (ie, Despite benign overnight monitoring on telemetry — there still is significant potential risk for subsequent development of prolonged bradycardia).
Additional PEARLS — can be found in my hour-long ECG Video on the Basics of AV Block.
- If you click on SHOW MORE (under the video on the YouTube page) — You’ll find a detailedtimed/linkedContents of all in this video.
- CLICK HERE — to go directly to the part (beginning at 30:09) that deals with the 3 types of 2nd-Degree AV Block.
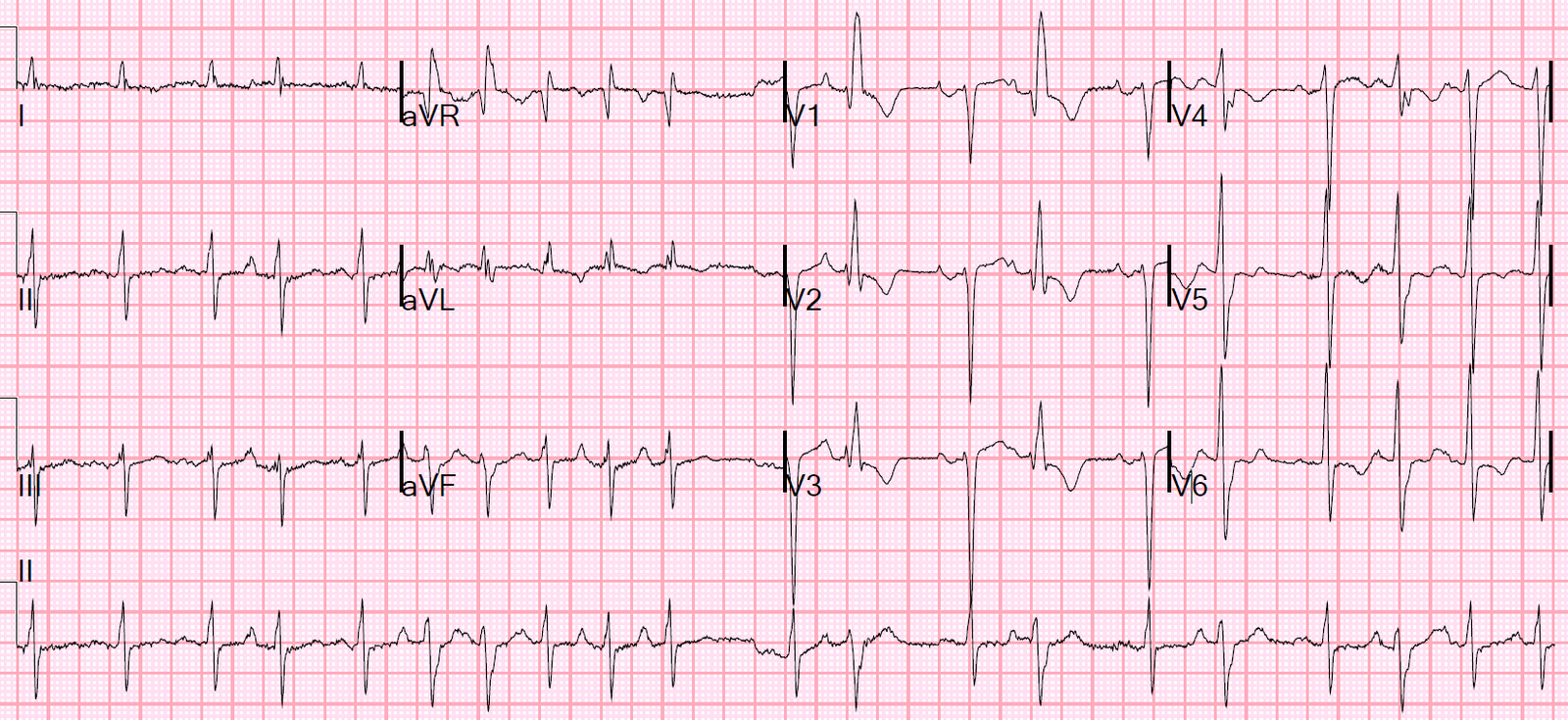
P.S. (1/2/2020): Since there have been some questions regarding atrial activity in this case (P waves are of low amplitude) — I am adding Figure-1, in which I have numbered the beats and labeled P waves.
- Calipers greatly facilitate establishing that P waves are quite regular here (perhaps with slight variation in some P-P interval).
- Calipers also verify that the PR interval is not increasing (ie, this is not Mobitz I ).
- PEARL: The best (easiest) way to tell if the PR interval during a sequence of beats is increasing — is to look at the PR interval just before the pause (ie, the PR interval before beat #2) — and compare this to the PR interval at the end of the pause (ie, the PR interval before beat #3). Do this for each pause in the tracing (ie, Compare the PR interval before beat #6 with the PR interval before beat #7). Note that there is NO difference between any of these PR intervals — thus, the PR interval remains constant throughout, and this is Mobitz II.
- The PR interval is not prolonged. The easiest way to measure the PR interval is to find a P wave on the rhythm strip that begins on a heavy line (BLUE arrow inFigure-1). Note that the QRS complex of beat #2 begins slightly before the next heavy line — which means that the PR interval is definitely not more than 1 large box in duration. This is a normal PR interval (Given the wide range of “normal” PR intervals — my preference is not to call 1st-Degree AV Block until the PR interval is at least 0.22 second in duration).
 |
| Figure-1: The ECG in this case (See text). |
![]()