Case 1
A 4 month old infant with known co-arctation of the aorta and reflux presented with respiratory distress.
Here is the ECG:
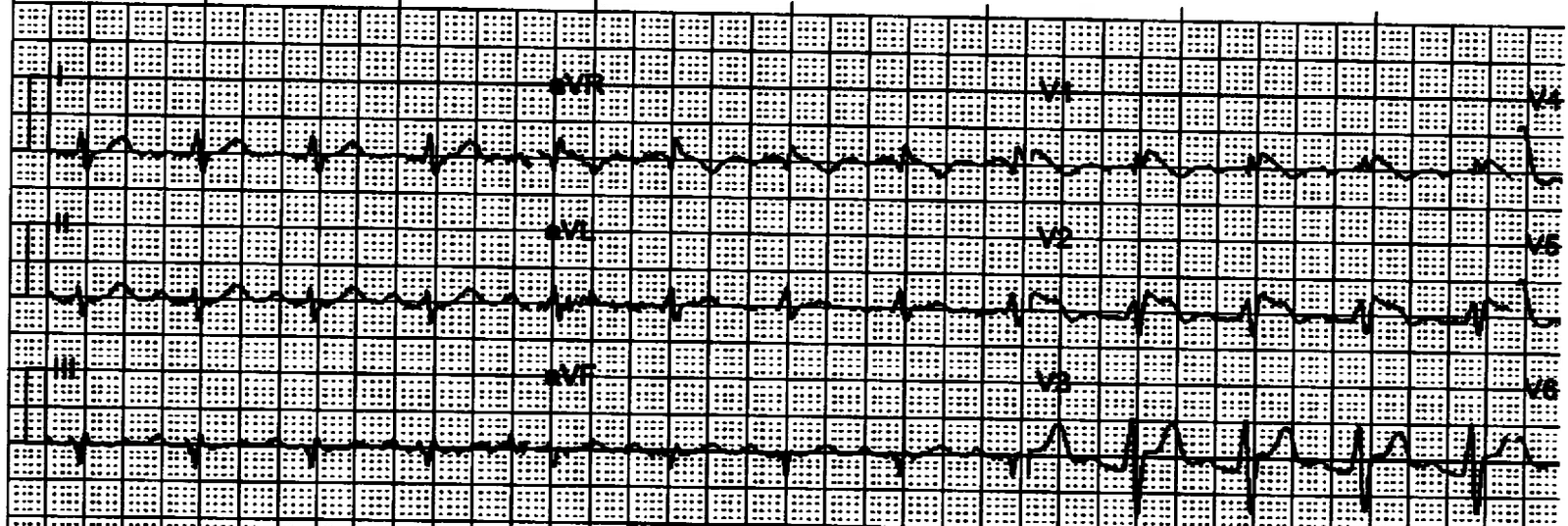
 |
| A Narrow Complex Tachycardia with a rate of 218. What is the rhythm? |
Answer: there are clear P-waves in nearly every lead. Notice the intervals are very short, which is typical of infants. Infants can have very fast sinus tachycardia, easily reaching a rate of 220. Most SVT in infants is faster than 220.
Throughout this case, the patient was on a cardiac monitor and the rate drifted up as high as 246, still in sinus (not recorded)!
The tachycardia turned out to be a result of disease (pneumonia), not a cause of it.
Case 2
This newborn presented to the ED for some exudate on the umbilical stump. There was no fever. The infant was very well appearing. The palpated heart rate at triage was 140. There were no respiratory symptoms.
The ECG was performed because, on auscultation, the heart rate was far higher than palpated by pulse.
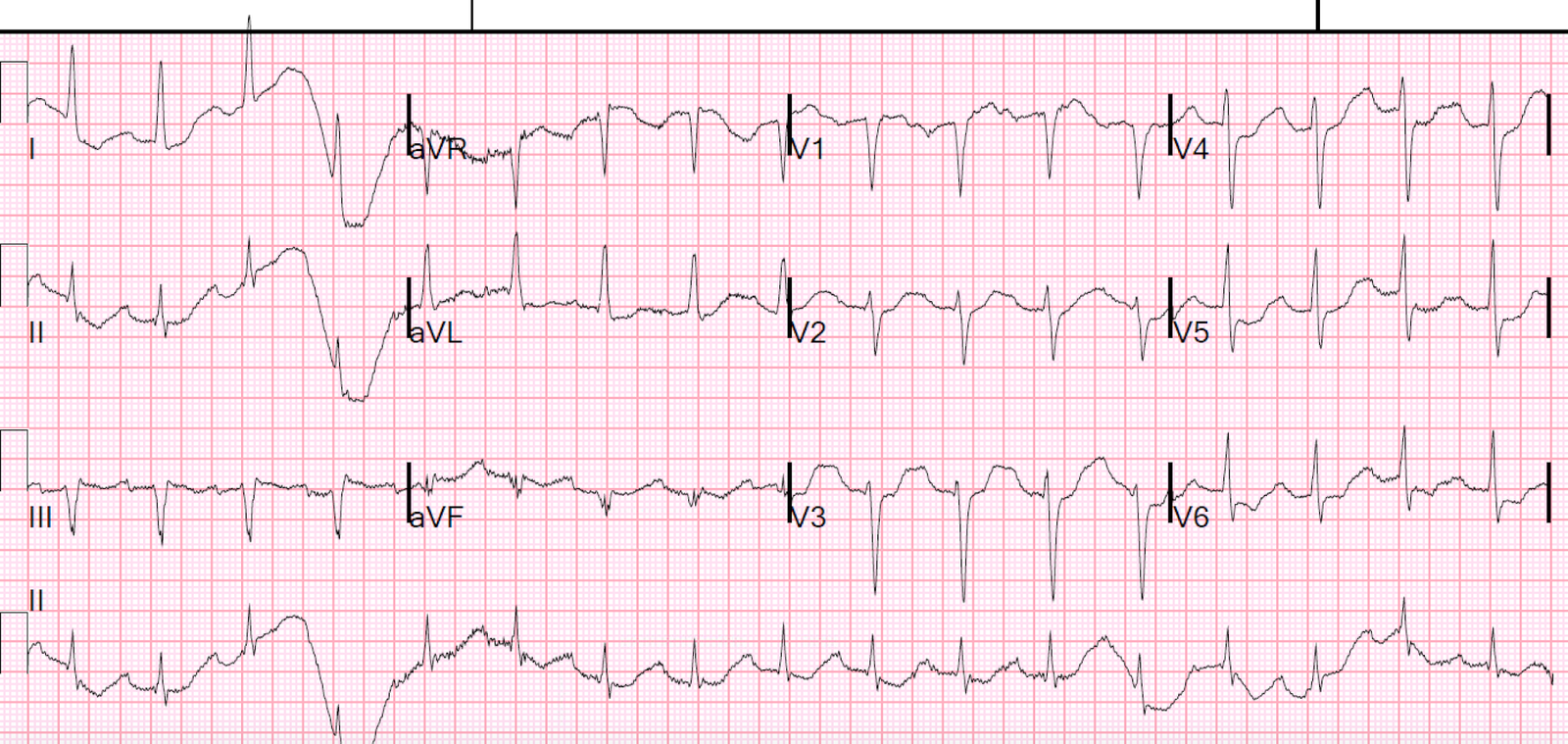
 |
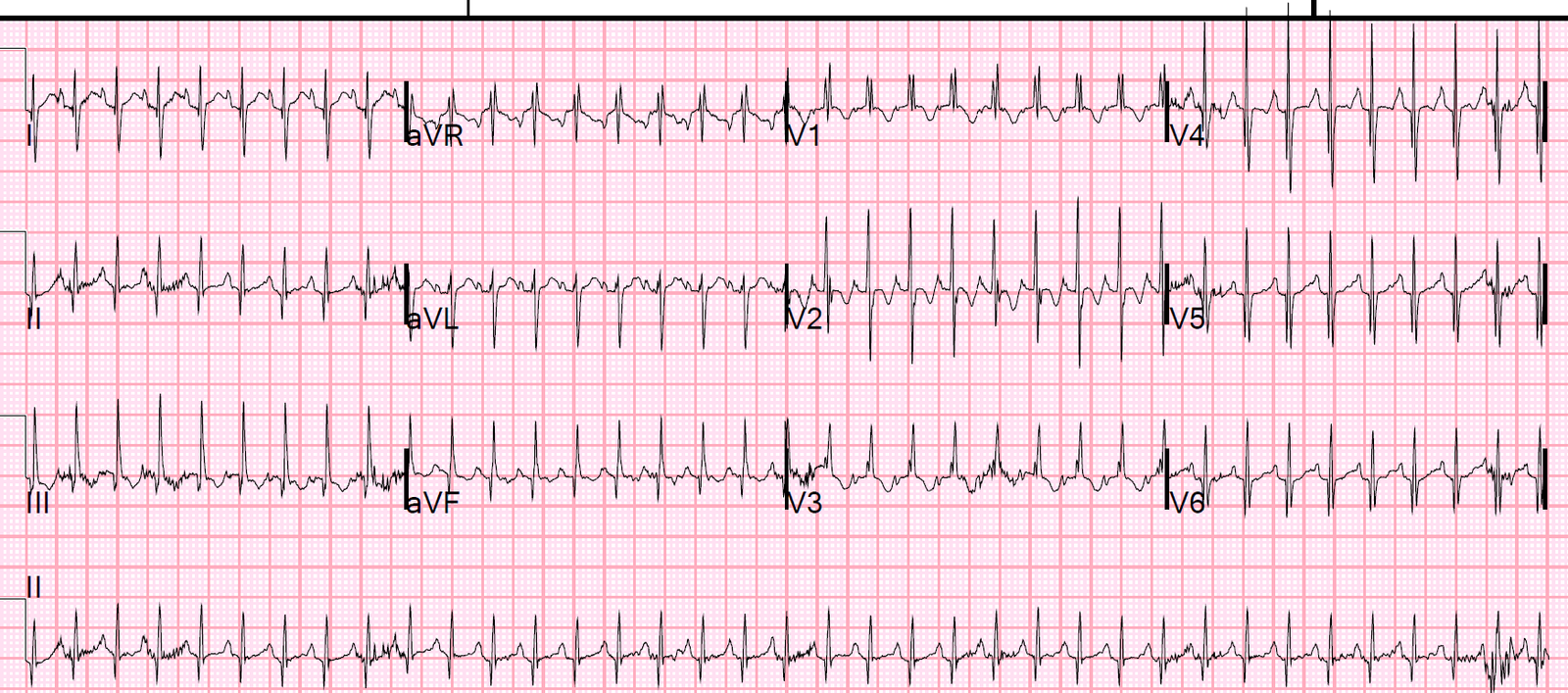
| Narrow complex tachycardia at a rate of 300. |
This shows how fast SVT can go in an infant and how well tolerated it might be. This infant was completely without any signs of illness.
There is also electrical alternans, which is a normal finding in PSVT.
If you see this in sinus tachycardia, it indicates tamponade.
It was converted to sinus with adenosine.
Learning points
This shows how well a newborn/young infant tolerates a very fast heart rate, and that sinus tachycardia of 218 is not unusual, and may even go as high as 240!
If in doubt, use Lewis leads to find otherwise hidden P-waves
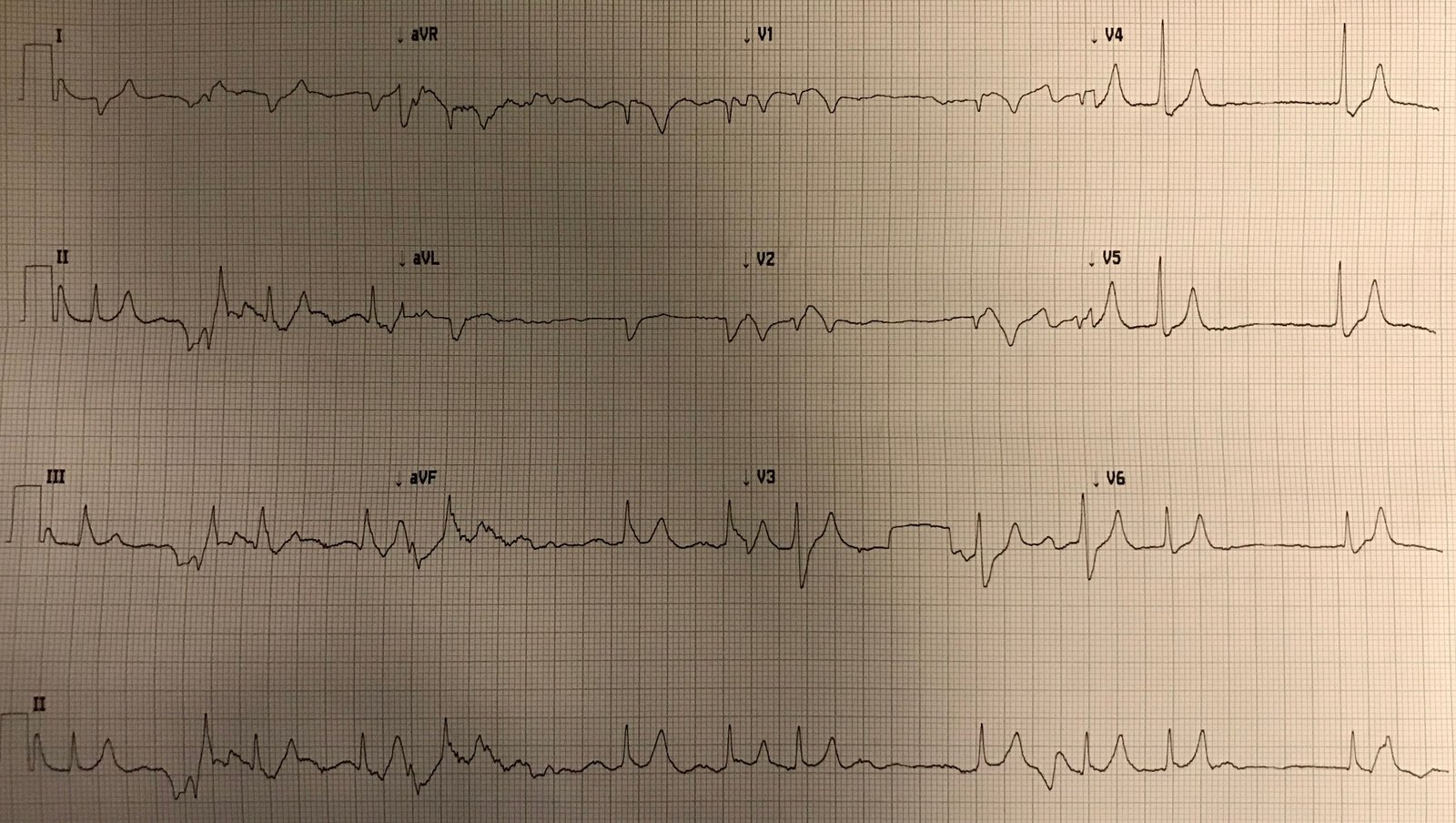
I don’t have a case of use of Lewis leads in pediatrics, but here is a nice one in an adult: