Submitted by Anonymous, written by Pendell Meyers
A woman in her 70s with HTN and DM had been experiencing lower chest / upper epigastric pain off and on for approximately one week until it acutely worsened, with diaphoresis and extreme fatigue. Her family called EMS and EMS recorded hypotension and this ECG:
 |
| What do you think? |
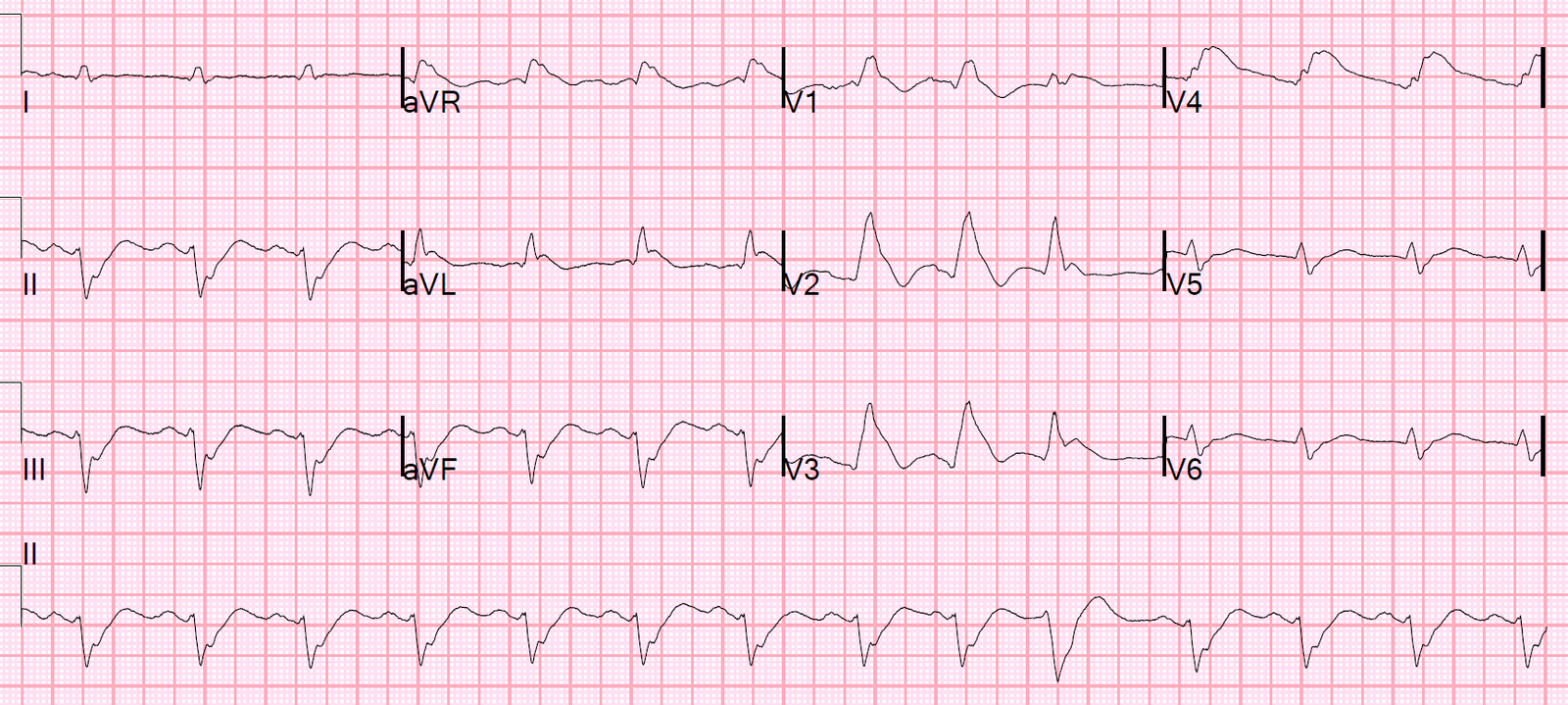
This is an obvious inferoposterior OMI. There is STE in III and aVF which does not meet STEMI criteria due to insufficient STE in lead aVF. There is reciprocal STD in I and aVL. There is STD in V1-V5, maximal in V2-3, which is diagnostic of the posterior component. The quality is not perfect, but I believe this is sinus rhythm at about 100 bpm with prolonged PR interval.
It is impossible to determine from this ECG if there is also a right ventricular MI, but there is a suggestion of RVMI: the STD in V2 is very deep and yet minimal in V1. STD in V2 from posterior MI can “pull down” the STE in V1 and negate it.
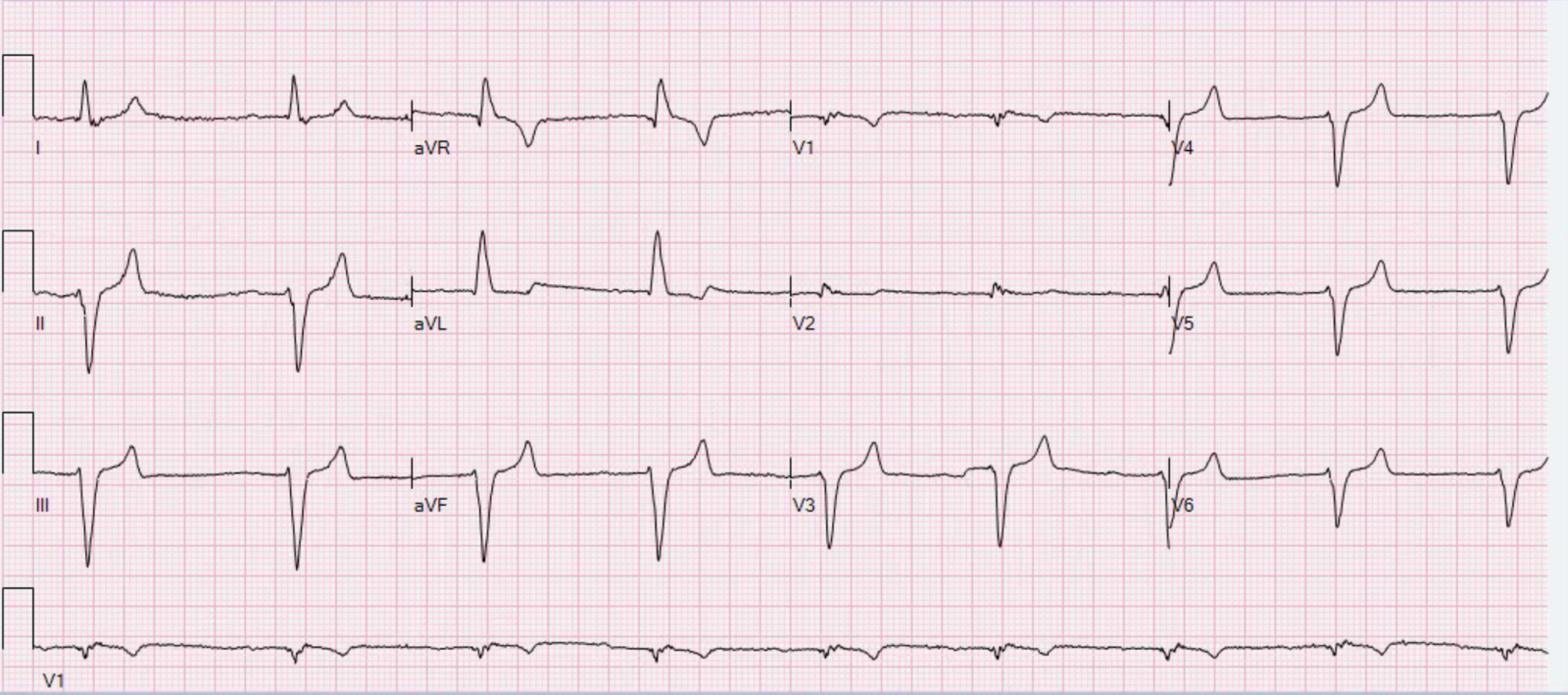
On arrival in the ED, she was profoundly hypotensive, nearly obtunded, and bradycardic. Resuscitation was initiated and this ECG was obtained:
 |
| Likely AFib (irregularly irregular) with bradycardia. ST changes persist, however this ECG shows some signs of reperfusion including terminal T-wave inversion in the inferior leads with tall posterior reperfusion T-waves in V2-4.
Of course, the electrical and mechanical aspects of reperfusion are not always perfectly coincidental – just because there appears to be transient electrical reperfusion pattern does not mean that the inferior and posterior walls (or the SA and/or AV nodes) are functioning. |
The cath lab was activated. The interventionalists insisted that the ECGs did not meet STEMI criteria and cancelled the activation, stating that they would consider urgent cath after further stabilization.
Atropine produced no response. The patient was placed on pressors and transcutaneous pads (which failed to capture). She was intubated and a transvenous pacemaker was inserted with good capture. She received PR aspirin.
Bedside echo showed obvious inferior wall motion abnormality and good TVP placement, no effusion.
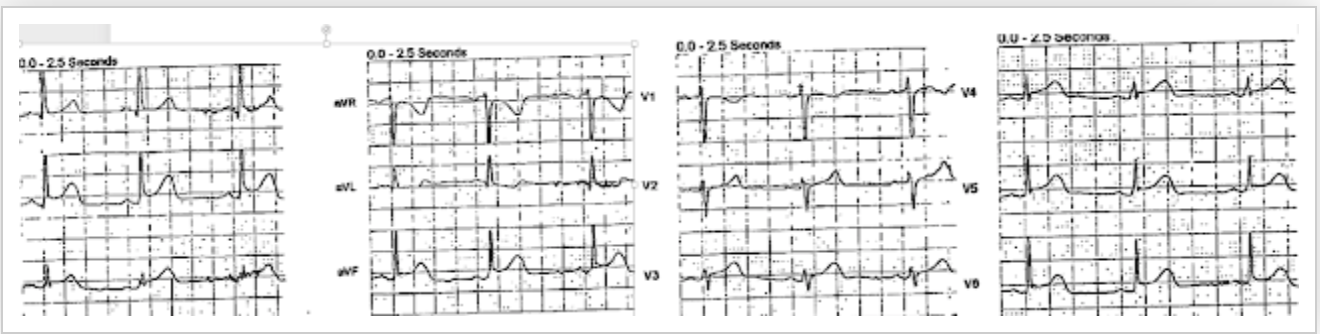
At about 30 minutes after presentation, the patient had acceptable vital signs with the TVP and low dose epinephrine drip. Another ECG was obtained during pacing:
 |
| Mostly paced rhythm with PVCs (#3, #6, #9, #12). The PVCs have obvious STE in III and aVF and V6, with STD in I, aVL, V2-3. The paced beats show a clear OMI pattern as well, by the modified Sgarbossa criteria: lead III for example has 3.5 mm STE with 9.5 mm QRS = 37%, well over 20-25% as we have described. Proportionally excessive discordant STE is present in II, III, aVF, and V6. V5 has a barely concordant appearance, probably not a full millimeter. |
The ED team again pointed out the evidence of inferoposterior OMI, this time by the modified Sgarbossa criteria. The cardiologists were not familiar with this and insisted that the ECG in paced rhythm could not be used to “look for a STEMI”. After some discussion, cardiology insisted that they would need a native rhythm ECG to evaluate for STEMI criteria.
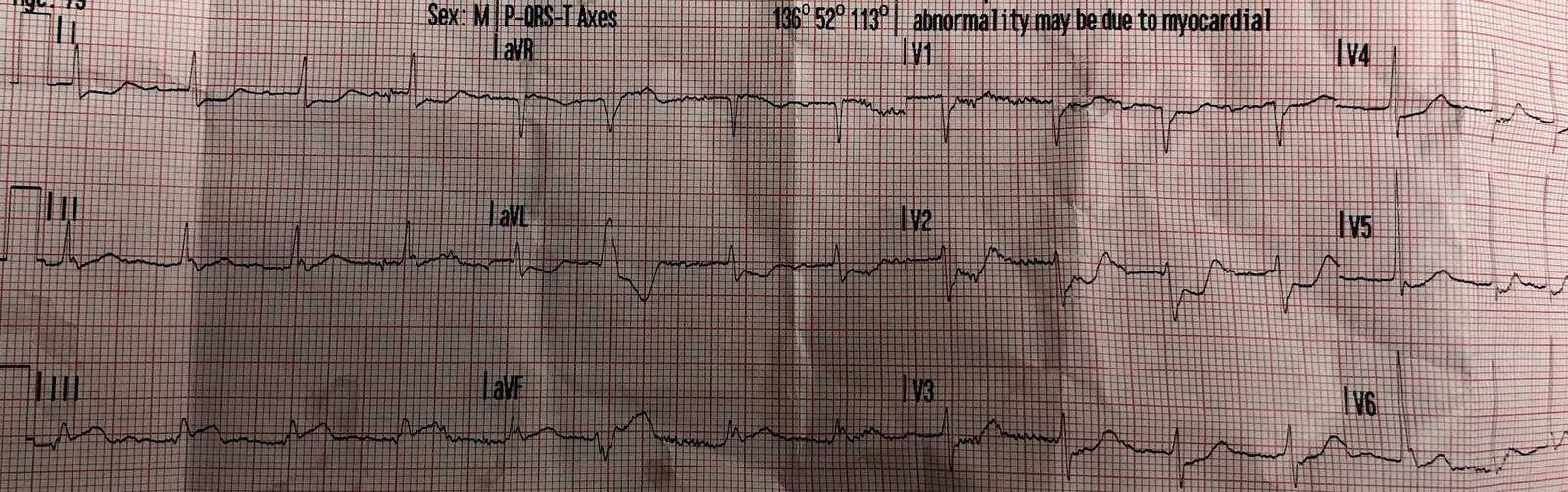
So they paused the TVP and obtained this ECG:
 |
| First beat is paced, then the rest are native. There appear to be very small possible P waves which may be conducting with huge PR interval and heart block, but this is irrelevant clinically. The QRS is narrow and shows a clear inferoposterior OMI pattern like all the ECGs before. |
The ED team believed that this ECG met STEMI criteria, however the cardiologists felt that there the inferior leads had significant J-waves at the J-point, followed by STE that does not meet STEMI criteria.
At this point it was approximately 90 minutes after patient arrival.
Cardiology requested a head CT before cath for unknown reasons, which was negative. First troponin T was positive at 0.06 ng/mL.
Cardiology then requested 2U PRBC transfusion for Hgb 7.5 prior to cath, which was started.
During this time, the patients blood pressure continued to decline, requiring 4 pressors to sustain hemodynamics.
The patient expired approximately 2.5 hours after arrival, before cath was performed.
Learning Points:
We must not let STEMI criteria prevent identification and/or treatment of Occlusion MI. We must hold ourselves and our consultants to a higher standard to protect our patients.
Use the modified Sgarbossa criteria to detect OMI in the setting of ventricular paced rhythm.
Consider thrombolytics for OMI when PCI is not an option.
![]()
===================================
MY Comment by KEN GRAUER, MD (1/19/2020):
===================================
There is a LOT to talk about regarding the series of tracings in this unfortunate case. I’ll limit my comments toward reinforcing concepts brought forth by Dr. Meyers — with additional focus on rhythm interpretation.
- I must respectfully disagree with Dr. Meyers regarding his comment that rhythm interpretation of ECG #4 is “irrelevant clinically”. On the contrary (as I’ll emphasize below) — more accurate rhythm interpretation would have provided one more way that the cardiology team could have (should have) been convinced that this patient was evolving an acute OMI in front of their eyes.
- For clarity — I’ll reproduce the 4 ECGs in this case.
- PEARL — As I’ve said many times before, use of Calipers is EASY, and it instantly makes you “smarter”. I had NO idea whether the atrial rhythm in ECGs #3 and #4 were regular — until I measured P-P intervals with calipers. This did not delay my interpretation — on the contrary, using calipers allowed me to accurately assess the underlying atrial rhythm much faster than trying to guess what might or might not be regular.
NOTE: Some of my comments below regarding rhythm interpretation are quite sophisticated ( = advanced). It is fine if you don’t follow them all — since it is the overall concepts that are important to enhancing and appreciating clinical interpretation of the essentials in this case.
 |
| Figure-1: ECG #1 — recorded by EMS on the scene (See text). |
Clinical Points Regarding ECG #1:
- I do not understand why the cardiology team was “stuck” on requiring “STEMI criteria” in this case. This 70-something year-old woman had symptoms for ~1 week prior to admission. While the additional history of “acute worsening” of symptoms might indicate the time of acute occlusion — given that she had symptoms for days prior to calling EMS — the cardiology team should clearly have considered the possibility that the initial event occurred before the day of admission to the hospital!
- The patient was hypotensive in association with the initial ECG ( = ECG #1). Regardless of whether “STEMI criteria” are (or are not) strictly met — a recent acute event in a dramatically symptomatic patient (this woman was profoundly hypotensive, with reduced mentation) is in-and-of-itself clear indication for prompt diagnostic/therapeutic cardiac catheterization.
- As per Dr. Meyers — ECG #1 shows an obvious inferoposterior OMI. There should be NO doubt that despite only 1mm of ST elevation in leads III and aVF — these are acute changes, given hyperacute ST-T waves in both leads III and aVF + mirror-image opposite ST-T wave reciprocal depression in lead aVL (further supported by 1 mm of flat shelf-life ST depression in lead I).
- Among the reasons why it may be that no more than 1 mm of ST elevation is seen in leads III and aVF are: i) That the QRS is tiny in these leads (as it often is with inferior MI) — so percentage-wise, the amount of J-point ST elevation is actually >25% R wave amplitude in leads III and aVF; and, ii) This patient’s symptoms have been ongoing for ~1 week — so some of the ST elevation may have receded by this point in the process.
- As per Dr. Meyers — there is very deep ST depression in anterior leads, that approach 3 mm deep in lead V2. Many experts view this shape of ST depression in one or more anterior leads as the “reciprocal” of what is ongoing in the LV posterior wall — which should (for practical purposes) translate to more-than-enough acute ST deviation to qualify for “STEMI criteria”.
- Dr. Meyers’ point regarding the possibility of associated acute RV involvement (because of no more than minimal ST depression in lead V1, in the face of marked ST depression in V2) — is extremely relevant in this patient with profound hypotension — since need for volume replacement is a prominent part of resuscitation. Right-sided chest leads would have provided a more definite answer regarding associated acute RV involvement.
- While not part of “written STEMI criteria” — the unexpected 2 mm of J-point ST elevation for the PVC in lead aVF of ECG #1 provides additional evidence of recent (and/or ongoing) acute OMI.
- Unfortunately — the quality of ECG #1 + baseline artifact prevent accurate rhythm interpretation. That said, I agree with Dr. Meyers that this most likely represents a sinus rhythm at ~95/minute + 1st-degree AV block — though we’d need a better quality rhythm strip to know for certain what the rhythm is. That said — Remember that we suspect 1st-degree AV block (this becomes relevant with rhythm assessment of subsequent tracings!).
 |
| Figure-2: ECG #2 — recorded on arrival in the ED (See text). |
Clinical Points Regarding ECG #2: I found the rhythm in ECG #2 especially interesting:
- I agree with Dr. Meyers that there is likely to be some underlying AFib in ECG #2 — because the R-R intervals preceding beats #3, 4 and 7 are all different — and we do not see clear sign of P waves in any of the 12 leads on this tracing.
- That said — note that QRS morphology changes in the long Lead V1 rhythm strip. Using Calipers allows you to instantly measure R-R intervals — and it is not by chance that the R-R interval preceding each of the 3 beats with incomplete RBBB morphology is identical ( = 8.3 large boxes in duration).
- This confirms that these 3 beats ( = beats # 2, 5 and 6) are escape beats. Since the QRS complex is no more than slightly prolonged for these 3 beats, with a very similar initial deflection that manifests incomplete RBBB/LPHB morphology (LPHB morphology is seen for beat #2 in simultaneously-recorded leads I,II,III) — the site of this escape focus is in the conduction system, most likely arising from the left anterior hemifascicle.
- In addition to marked bradycardia — could there be high-grade AV block? Intermittent conduction defects (such as the incomplete RBBB/LPHB seen here) — are most commonly associated with acceleration of the heart rate — yet they are seen here with increased bradycardia — which leads me to suspect a progression of AV block in this patient with ongoing and evolving inferior MI. Acute inferior MI is notorious for its association with stepwise progression from 1st-degree — to 2nd-degree AV block, Mobitz I — to 3rd-degree AV block — and perhaps we are seeing this?
 |
| Figure-3: ECG #3 — recorded after ~30 minutes in the ED, after placement of a transvenous pacemaker (See text). |
Clinical Points Regarding ECG #3:
- As per Dr. Meyers — ECG #3 shows a paced rhythm with ventricular trigeminy (every 3rd beat is a PVC).
- Using Calipers allows you to establish an underlying regular atrial rhythm! I’ve highlighted with RED arrows in ECG #3 those low-amplitude P waves that I am nevertheless certain about. Following through this P-P measurement with my calipers, allows detection of the likely remaining P waves (PINK arrows).
- I suspect the mechanism of this rhythm is not sinus — because we really don’t see atrial activity in lead II (therefore, an ectopic atrial rhythm is likely).
- While hard to diagnose coexistent underlying AV block given regular ventricular pacing in ECG #3 — the fact that the PR interval constantly changes, but without any evidence of conduction suggests there is some underlying AV block (probably high-grade 2nd-degree).
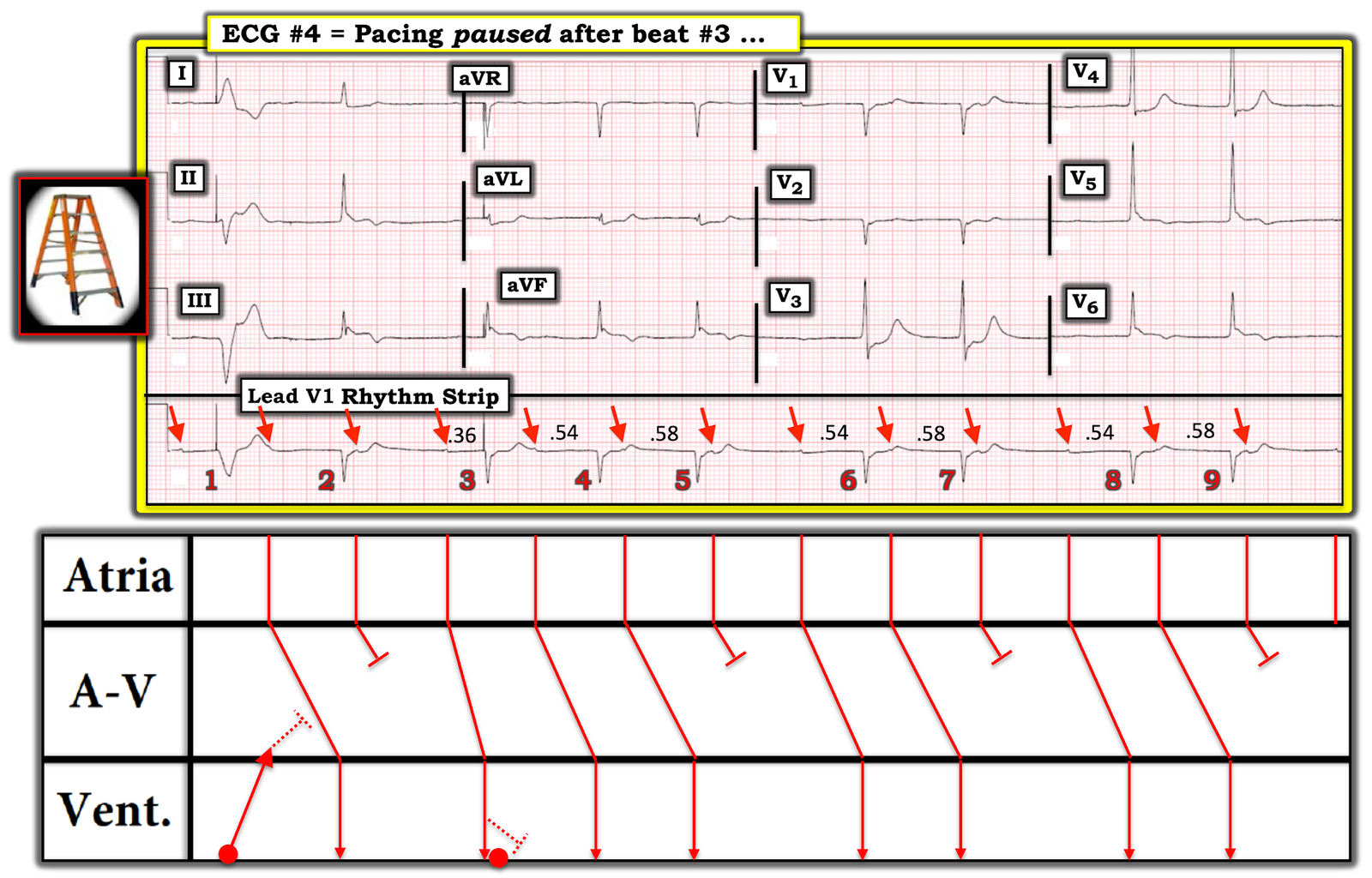 |
| Figure-4: ECG #4 — recorded by the cardiology team after pausing pacing after beat #3 (See text). |
Clinical Points Regarding ECG #4:
- IF you were skeptical about my statement that there is an underlying regular atrial rhythm in ECG #3 — then review of ECG #4 should resolve any skepticism. There can be NO doubt that regular (albeit non-sinus) atrial activity is evident in ECG #4 (RED arrows).
- There can also be NO doubt that 2nd-degree AV block, Mobitz Type I (ie, AV Wenckebach) is present in ECG #4. There is group beating — with the R-R interval between beats #6-7 and #8-9 being identical — and then with the preceding R-R intervals (between beats #5-6 and between #7-8) also being identical. The PR intervals preceding beats #4, 6 and 8 are all identical ( = 0.54 second) — with identical PR intervals for the 2nd beat in each of these groups ( = 0.58 second). There is NO way this is by chance!
- NOTE: Two pacing spikes are seen in ECG #4 — and this resets some of the PR interval relationships. Beat #1 is paced (Note the very wide and different-looking QRS complex). We also see a pacing spike just in front of beat #3 — but since the QRS complex of beat #3 looks identical to that of all other beats on this tracing — I postulated that beat #3 was conducted with a PR interval = 0.36 second.
BOTTOM Line: While some details about the rhythm in ECG #4 are less than certain — there can be NO doubt that 2nd-degree AV block, Mobitz Type I is present in ECG #4 — in this 70-something woman with ~1 week of symptoms (with recent exacerbation) + clear evidence of ongoing acute infero–posterior (probably also RV) OMI.
- Recognition of the rhythm disturbances in this case is relevant (in my opinion), since what appears to be 1st-degree AV block — then high-grade 2nd-degree AV block — then clear evidence of Mobitz I — is so characteristic of AV conduction disturbances seen with evolving inferior OMI, as to supply further confirmation that there has been a recent acute cardiac event that is still ongoing.
- CONFESSION: I do not understand why the cardiology team involved in this case refused to cath this profoundly symptomatic patient.
- I hope feedback is provided to the involved cardiology team …
![]()