A young previously healthy man with no past medical history presented with a complaint of epigastric pain for a few days. He had no other complaints. He appeared well. Vitals were HR 107, BP 140/70, sats 98%, RR 20, Temp 36.7.
He had a normal exam except for the mild tachycardia.
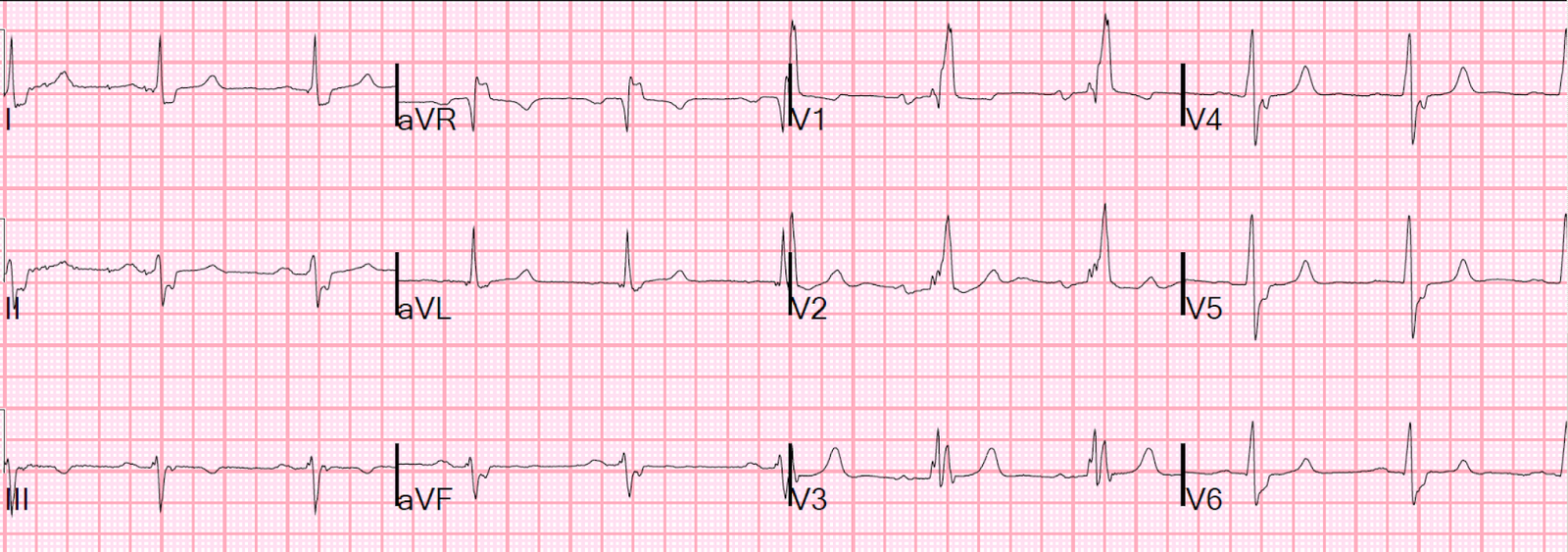
The physician was planning on discharging the patient except for the tachycardia, which prompted him to obtain an ECG. He was startled by the result. He showed it to me:
 |
| QRS 105 ms. Sinus tach. RV conduction delay (R’-wave in V1) Diffuse ST depression, diagnostic of ischemia. |
Not knowing anything else about the patient, I just said, “This is ischemic ST depression. He is seriously ill.”
He denied any chest pain, shortness of breath, vision changes, numbness, tingling, weakness in upper or lower extremities, neck pain or stiffness, or urinary symptoms. He had no personal or family cardiac history. He had no calf pain or swelling, no recent surgery or travel, no history of clot or hemoptysis. He stated he was working too hard and not drinking enough water.
They did more workup.
He started to complain of a mild sore throat and headache. A test for group A Strep was positive. A troponin I returned at 0.454 ng/mL. Perhaps myocarditis?
Fluids were given for presumed dehydration.
The patient then became very SOB. He spiked a fever. He went into respiratory failure. He was intubated. Here is his chest X-ray:
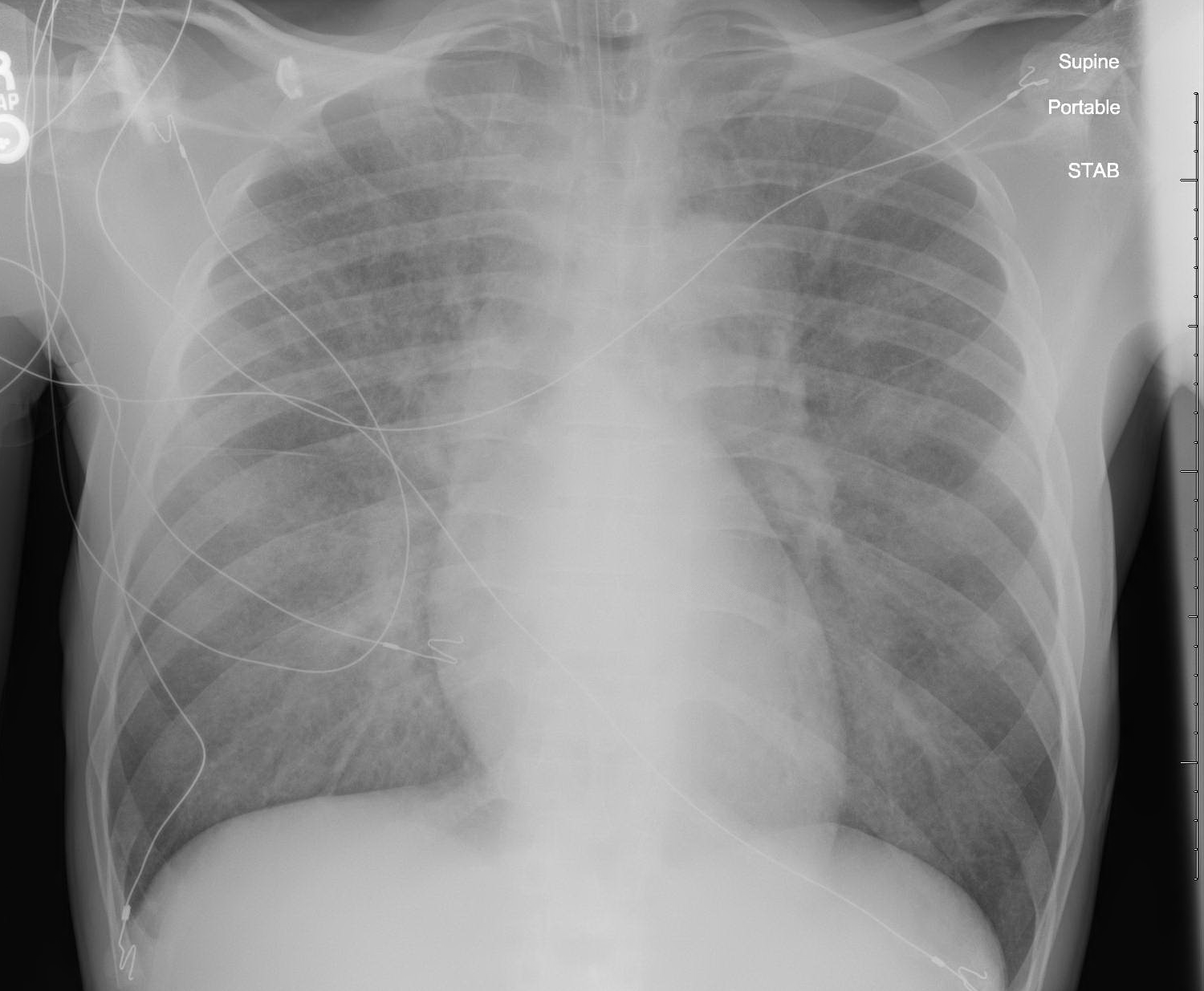 |
| Pulmonary Edema without cardiomegaly |
A bedside echo was done:
There is hyperdynamic function. There is no evidence of myocardial dysfunction or decreased contractility. There is no apparent reason for cardiogenic pulmonary edema.
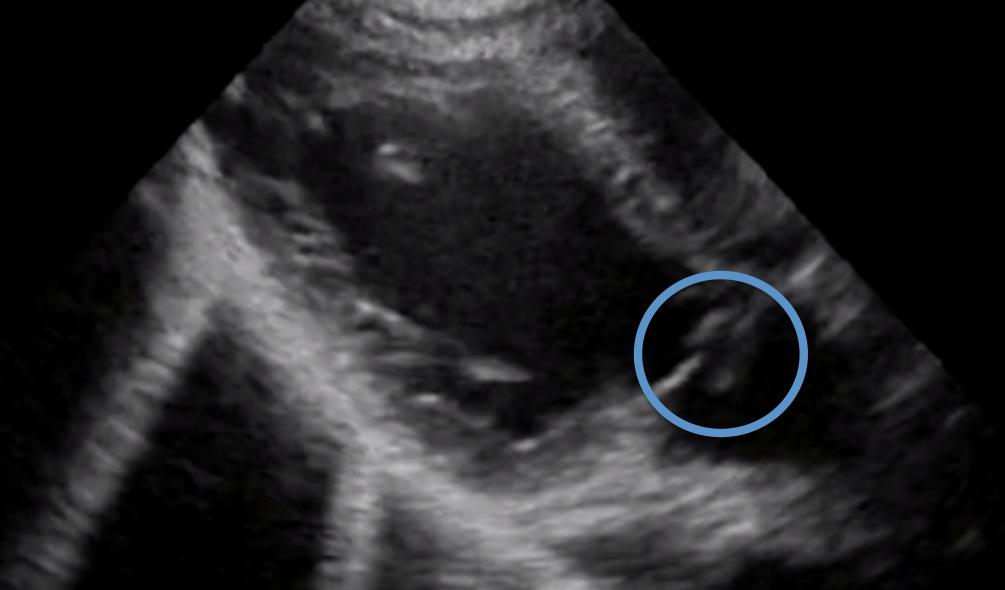
Here is another view:
There is a finding here that could make the diagnosis if you are looking for it and are good at reading ultrasounds.
It may be seen on this still capture of the video below:
 |
|
|
This was not seen and Doppler was not done (until a much later formal echo). What is the probable diagnosis?
The diagnosis was aortic valve endocarditis with severe aortic regurgitation. Blood cultures were positive for a common organism.
I cannot give more information without compromising patient confidentiality, but no more is needed to make the point.
Learning points:
1. An ECG can often find serious cardiac pathology when none is suspected.
2. ST depression is most often due to demand ischemia, less often due to acute coronary syndrome
3. “Positive” troponins have many etiologies
4. Most important: A hyperdynamic heart on cardiac echo does not rule out heart failure or cardiogenic shock: acute valvular failure is too often forgotten as the etiology.
And don’t forget tricuspid regurgitation as an etiology of right heart failure. We have seen two cases of acute tricuspid insufficiency from trauma (sudden compression of heart during systole rupturing chordae to tricuspid).