A healthy 20 y.o. man presented with lightheadedness.
There are great comments I’ve now posted at the bottom from Ken Grauer and Jerry Jones.
The symptoms began about 2 weeks prior and were exertional. He stated that he plays on a college basketball team and he noticed over the previous 2 weeks that every time he exercised with the team he felt lightheaded.
There was no actual history of syncope. He had had no associated chest pain, shortness of breath or palpitations. He had had no symptoms at rest or associated with positional changes. No history of similar symptoms previously. No history of heart or lung disease. There was no family history heart problems, sudden death, drowning, deafness. He did not take any medications.
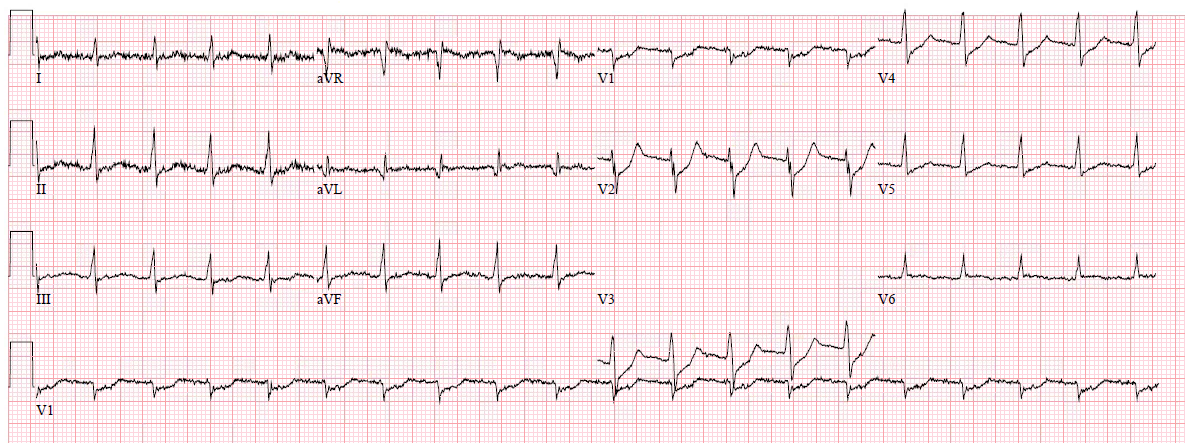
Here is his ECG:
 |
| What do you think? The treating physicians diagnosed complete AV block. |
There is a narrow complex bradycardia at a rate of about 42. It is hard to determine if there is a P-wave before the first complex, as that complex is at the edge of the tracing.
The 2nd complex definitely does NOT have a P-wave in front, nor does the 3rd or 4th. However, the 5th has a P-wave which is followed very shortly (at less than 120 ms) by a QRS. The 6th has a slightly longer PR interval, and the 7th and 8th longer still.
The longest of the PR intervals is the 7th.
What is this rhythm? Is there AV block?
No! At least we see no evidence of block here. There is no P-wave which does not conduct. This is AV dissociation. But not all AV dissociation is due to AV block. In this case, it is “Isorhythmic Dissociation.” The sinus node and the AV node just happen to be discharging at the same rate, and also coincidentally are happening at about the exact same time.
The AV node is too impatient to wait for the sinus beat to conduct.
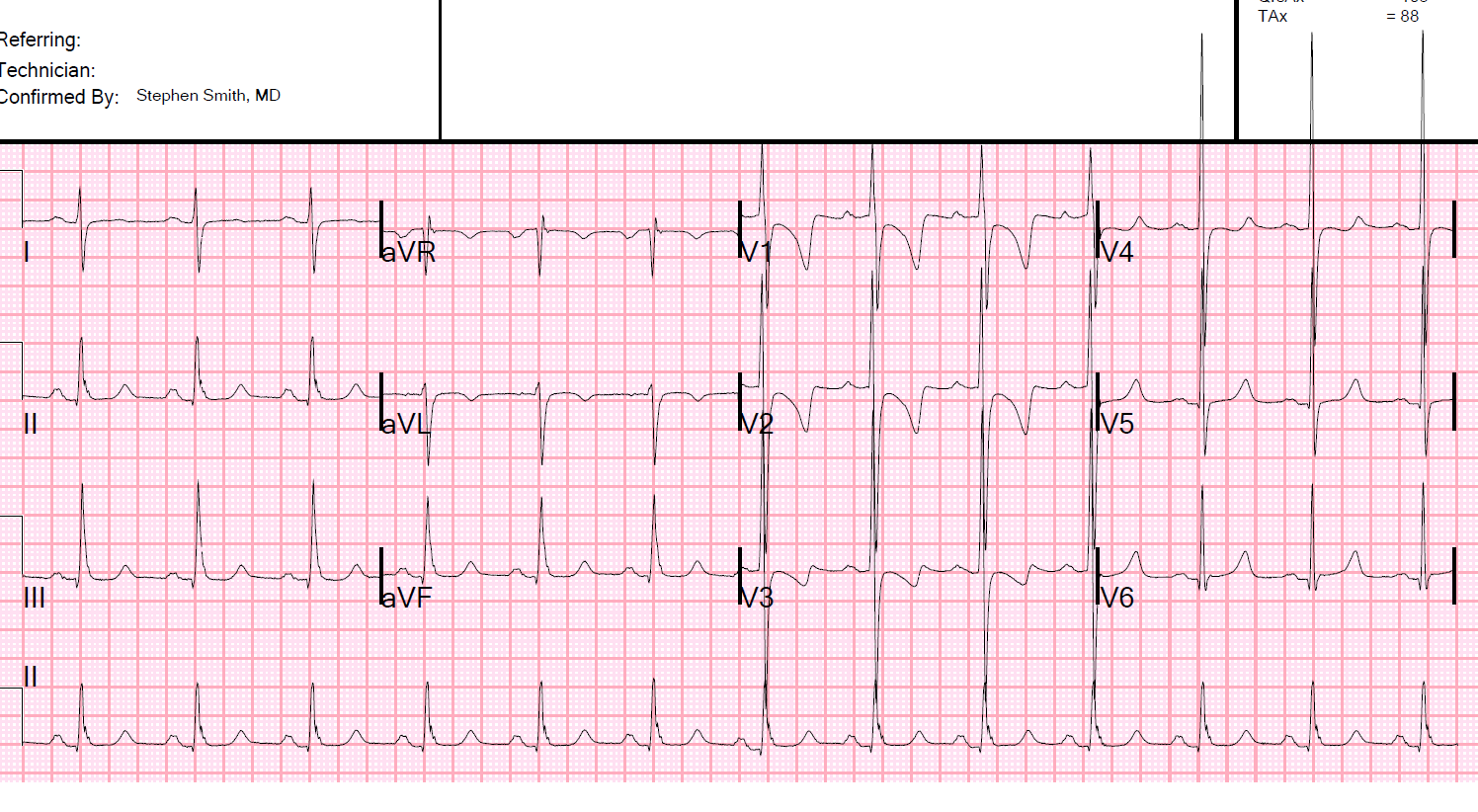
Let’s look at it again with annotation:
 |
|
The P-wave in complex 7 probably conducts (red line is PR interval). But I cannot prove this! The black lines in complexes 6 and 8 are exactly the same length as the red line in the 7th. You can see that the QRS initiates before the end of the black line in 6 and 8. Thus, the AV node is firing before the impulse from the sinus node had a chance to arrive. So the AV node was too impatient to wait for AV conduction. For complexes 2, 3, and 4, the P-wave is hidden in the QRS. Complex 5 has a preceding P-wave, but the very short PR interval makes it obvious that the QRS fired before that sinus impulse had a chance to conduct. |
Beyond rhythm, the ECG is completely normal for a young man, with early repolarization (see classic J-waves in II, aVF, V4-V6)
Could there be AV block? Yes, it is possible, and we cannot disprove AV block based on this ECG. But we have no reason to think there is AV block.
If the AV node is firing, why are there no retrograde P-waves? Because the sinus node fires before the impulse from below can reach the atrium. The ascending impulse from the AV node meets the descending impulse from the sinus node and they block each other.
How could we demonstrate absence of AV block? Just have the patient do a bit of exercise to increase his sinus rate to a rate faster than the AV node rate.
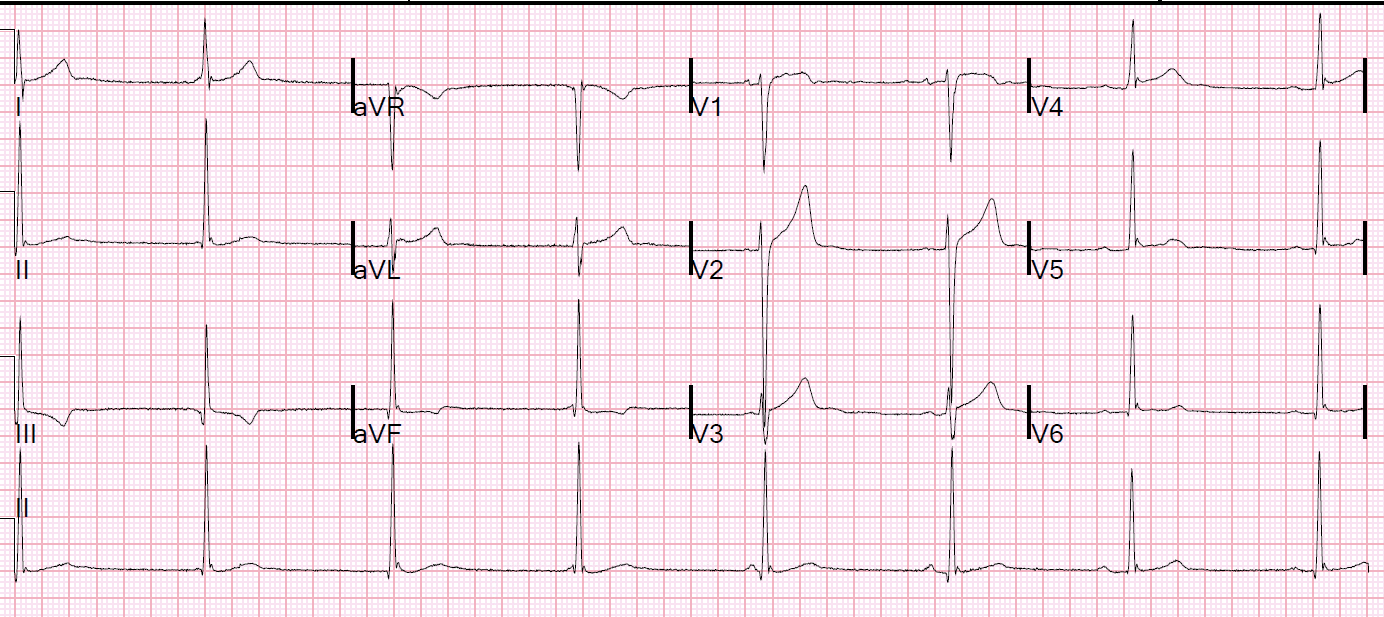
Another ECG was recorded later in the ED:
 |
| There is a slightly faster sinus rate now, almost 50, and now all P-waves are conducting. This shows that the J-waves were indeed J-waves, not hidden P-waves |
Clinical course:
The patient was admitted because of concern for intermittent complete AV block.
A walk test showed appropriate responsiveness of the sinus node with good AV conduction.
An echo was normal.
Learning Point:
1. Complete AV block is only one etiology of AV dissociation. Isorhythmic dissociation is another.
2. Isorhythmic Dissociation is a benign condition.
Here is a very nice article on AV dissociation:
https://emedicine.medscape.com/article/151715-overview
Here is a nice article on Isorhythmic Dissociation:
http://circ.ahajournals.org/content/circulationaha/42/4/689.full.pdf
Here is a nice example of Isorhythmic Dissociation with a Laddergram:
https://www.ecgguru.com/ecg/isorhythmic-v-dissociation
Here are other examples of Isorhythmic Dissociation:
Sudden weakness with bradycardia and bizarre T-waves
What is this rhythm?
AV Dissociation. Is there AV block?
Here are other posts on AV dissociation and AV block
AV Dissociation Lecture by K. Wang (28 minutes)
A Mystery Rhythm, Explained by K. Wang’s Ladder Diagram.
Another Guest post from K. Wang: What is the rhythm/conduction problem?
What Kind of AV Block is This? Guest Post by Dr. K. Wang (The Rhythm Master), Using a Ladder Diagram
Atrial Flutter. What else?? (AV dissociation with block)
Great comments from Jerry Jones and Ken Grauer:

Steve…
Great case! In my classes I emphasize recognizing the difference between 3rd degree AV block and simple AV dissociation because the implications and the resulting workup and treatments are so different. It’s unfortunate how many people interpreting ECGs think 3rd degree AV block is defined by AV dissociation (obviously, it isn’t!).
I do take issue with the sentence “There is no P-wave which does not conduct.” Actually, there is only one P wave that conducts (the capture beat) and it results in the slightly shorter R-R interval toward the end. I think a better way to phrase the sentence would be that “there is no P wave that failed to conduct that did not have an obvious reason for not conducting.” All but one P wave arrives at the AV node or His bundle during the effective refractory period. As you well know, it isn’t the AV dissociation that defines 3rd degree AV block – it’s the failure of a P wave to conduct when there is no reason for it NOT to have conducted.
This is, indeed, isorhythmic dissociation but it is sometimes referred to as dissociation by interference (the other two types being dissociation by default and by usurpation). What’s unusual here is that the atrial rate is slightly faster than the ventricular rate which is a situation typically seen with 3rd degree AV block. You can, however, see this in the interference type of AV dissociation. So the old adage that “if the atrial rate is faster than the ventricular rate, then it must be 3rd degree AV block” is simply not always true.
Thanks for a very informative and educational site.
-
ECG InterpretationMay 14, 2018 at 10:09 AM
Hi Jerry. This tracing is even more complex than it at first seems. Although in the 1st ECG, the sinus P wave rate is faster than the junctional escape rate toward the end of the tracing — I believe it most probably was SLOWER before these last few beats in the 1st ECG. Closely comparing QRS morphology of the escape beats to me suggests that a sinus P wave occurs just before onset of the QRS of beat #4; and just after the QRS of beat #3. I think the very slight elevation of the notch at the end of the QRS of beat #2 is due to the occurrence of a sinus P wave, which (if I am correct), would indicate that the sinus rate was indeed SLOWER than the junctional escape rate earlier on in the tracing. Of note — P wave morphology preceding the last beat ( = beat #8) in this 1st ECG is different (ie, flatter) than sinus P waves — which I believe is due to takeover by a low atrial rhythm. I believe this premise is supported by the 2nd ECG, for which P wave morphology in the long lead II is clearly different (flatter and notched) compared to P wave morphology in the 1st ECG for the sinus P waves. So as I suggested in my earlier Comment (from May 12) — I think the underlying rhythm in this case is marked sinus bradycardia + sinus arrhythmia — which results in switch of the pacemaker site between EITHER an AV nodal escape focus at 42/minute OR a low atrial escape. What remains to be shown (stated, but not documented in the initial presentation) — is whether there will or will not be an appropriate response to exercise in this previously healthy 20-year old who did present with exertional symptoms of “lightheadedness” (which of course is not “normal” for a 20-year old). THANKS as always for your insightful comments! I thought this was a GREAT case for discussion!

Jerry JonesMay 16, 2018 at 5:26 PM
Hi Ken! Always great to hear from you and get your input. I agree that this is a very complex tracing but I want to avoid reading too much into it. I think you are absolutely correct in that this is a sinus brady with sinus arrhythmia that has been usurped by a junctional pacemaker, most likely arising in the His bundle rather than the AV node or NH transition. While a focal ectopic atrial tachycardia is not that uncommon, an atrial escape rhythm is very, very uncommon – mainly because whatever (probably parasympathetic input) is causing the sinus brady almost always has the same effect on the areas of the atria with escape pacemaker activity. A junctional pacemaker in the His bundle would be affected very little – if at all. Regarding the conduction of the sinus (or atrial) impulses, after reviewing the first tracing again, I think there is a very strong argument that only the last two P waves conducted and they may even be P’ waves (certainly the last one is, as you pointed out). I don’t think the 3rd-from-last P wave conducted because – using my calipers – the QRS that follows it is right on time for the junctional escape rhythm. Plus, even though the PR interval is 0.20 seconds, that is not enough time for this AV node to conduct. The last two PR intervals are visibly longer than 0.20 seconds and so are the PR intervals in the final ECG. There are two kinds of “normal” PR intervals: the textbook normal (0.12 – 0.20 sec) and then whatever is “normal” for the patient. The last two QRS complexes are definitely out of sync with the junctional rhythm, so I think they were conducted. To say the 3rd-from-last QRS conducted, one would have to rely on coincidence and I always try to avoid invoking magic, divine intervention and coincidence as an explanation for a dysrhythmia. Admittedly, this can be difficult at times!
ECG InterpretationMay 20, 2018 at 3:40 PM
Hi Jerry. Thanks for your additional comment. Just to clarify — I never said (or meant to imply) that beat #5 was conducted — on the contrary, NOT only the shorter PR interval, but also the different QRS shape of this beat #5 (compared to beat #6 which IS conducted, and which manifests a shorter R wave) indicates that beat #5 is NOT being conducted. My point was simply that as uncommon as atrial escape rhythm might be in this setting — the change in P wave shape for this last beat (beat #8) in ECG #1, together with this same different (smaller, notched) P wave shape for each of the beats that are conducted in the 2nd tracing to me suggested that in addition to junctional escape — there was also an atrial escape rhythm occurring. As I believe we both believe — more monitoring would be needed to clarify this — and the clinical relevance of what we see will only be determined once we can determine if there is or is not an appropriate response to exercise in this previously healthy 20-year old who did present with exertional symptoms of “lightheadedness”. THANKS as always for your thoughts!