A young woman was found down, unresponsive, with legs crossed. She was intubated by medics. A prehospital EKG (not found, but reportedly identical to the first ED ECG below) was read as ***STEMI*** and after prehospital cath lab activation, the patient was transported to the ED.
On arrival, she was mechanically ventilated and not in apparent shock. Here is the ED ECG:
 |
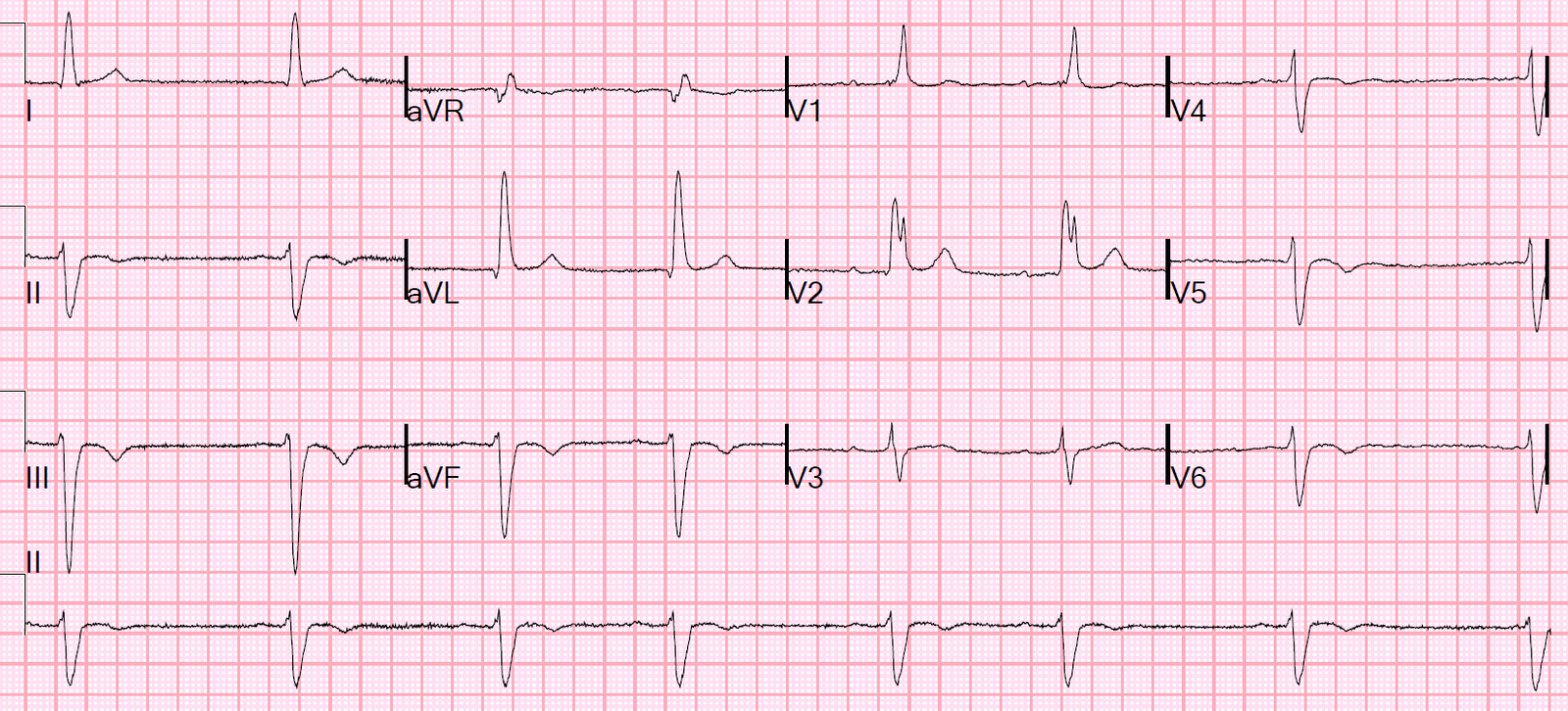
| This is a pathognomonic ECG. The computer reads the QRS duration as 133 ms. I have posted several of these in the past. What is it? |
Answer: it is pathognomonic of severe hyperkalemia. The downsloping ST elevation in V1 and V2, which resembles Brugada pattern, is not typical of STEMI, but is typical of hyperkalemia. Along with the prolonged QRS and pathognomonic T-wave peaking in I, II, aVL, and V4-V6, it is diagnostic of hyperkalemia.
Cardiology was consulted, hyperkalemia was considered, as well as tricyclic overdose. Calcium and bicarbonate were given.
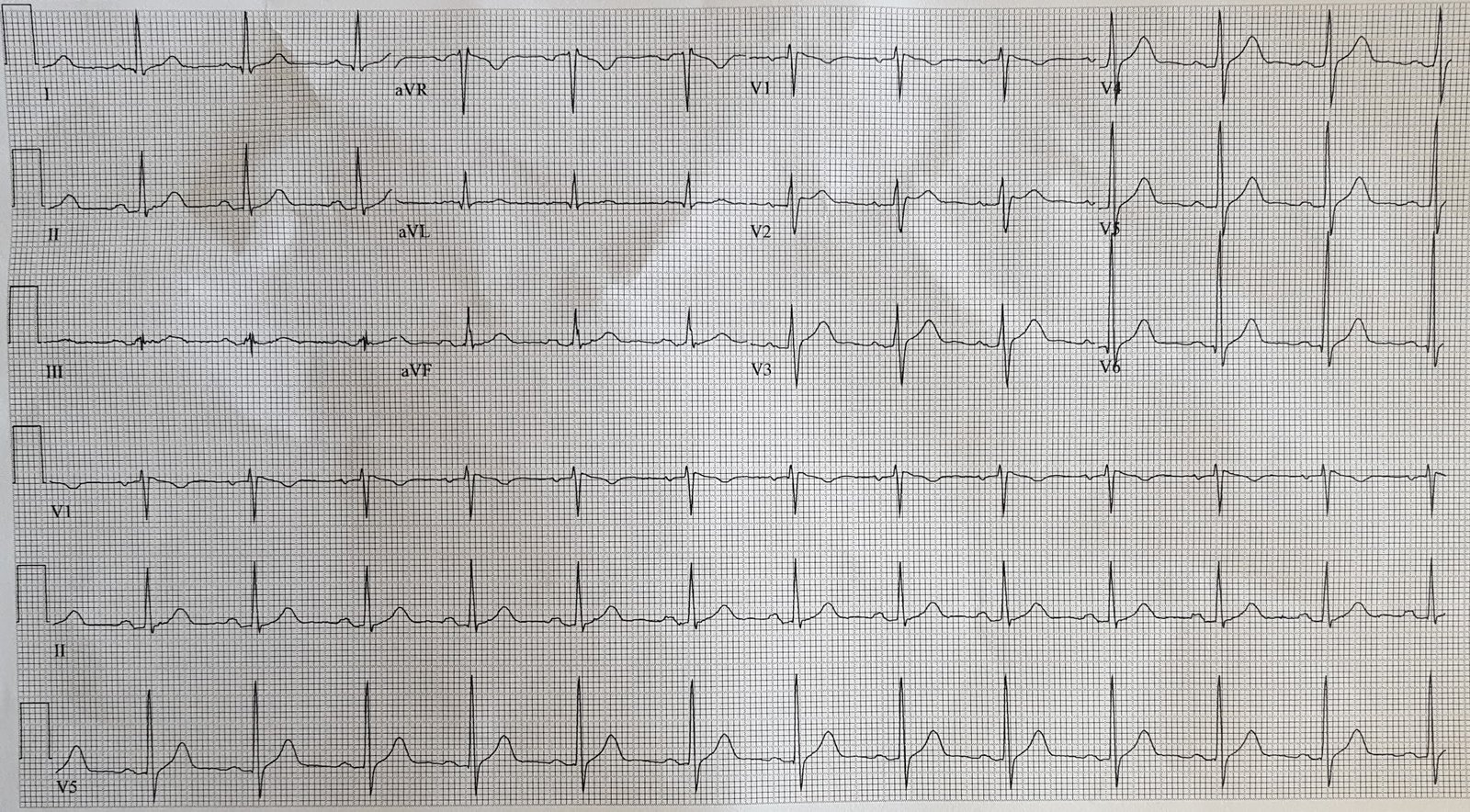
A repeat ECG was recorded 20 minutes after the first:
 |
| The QRS is now 125 ms. |
Subsequently, the K returned at greater than 9.4 mEq/L (unmeasurably high). There was a pH of 7.09 with both mild metabolic and mild respiratory acidosis, but without an elevated anion gap. The lactate was 8.9 mEq/L. Cr was 2.94 mg/dL.
The patient was found to have a compartment syndrome of the lower leg.
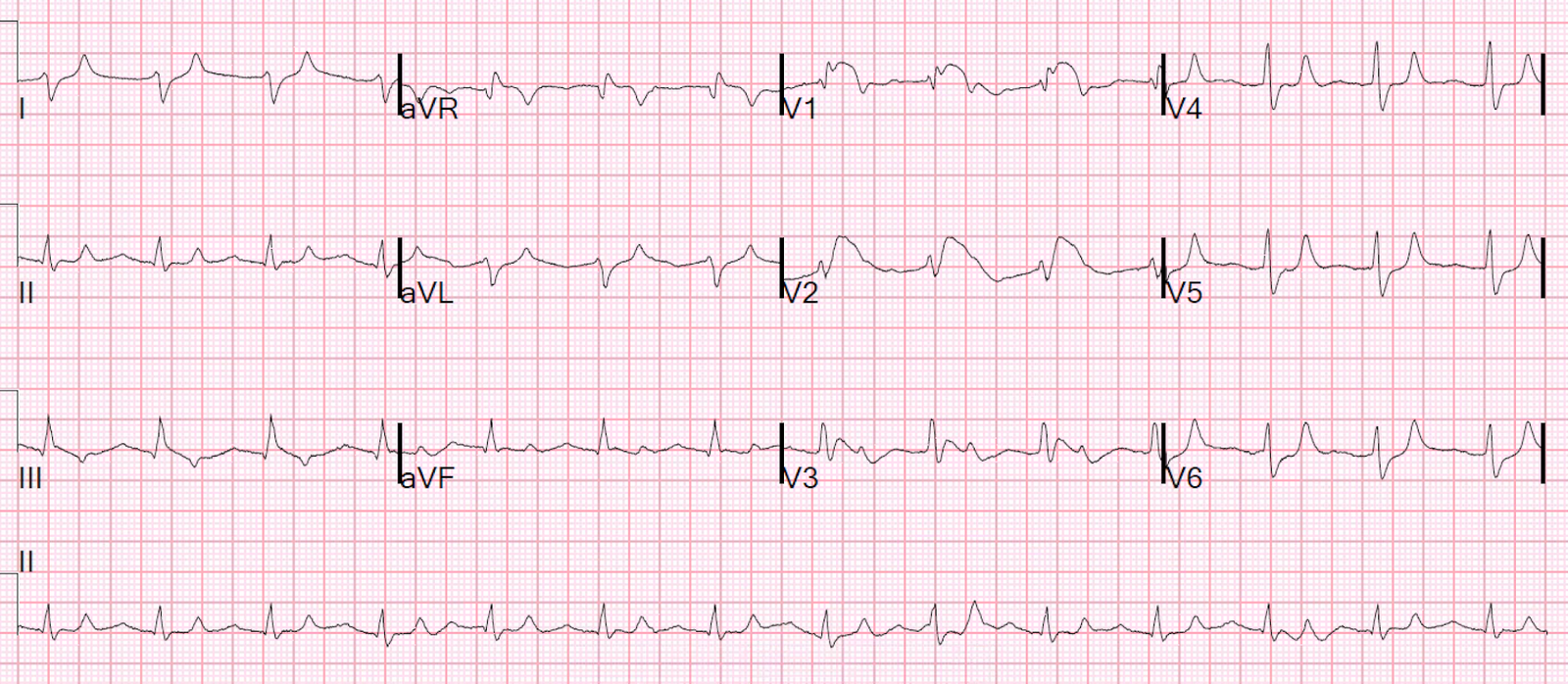
The K was further shifted with insulin, albuterol, insulin and dextrose, and another ECG was recorded at 2 hours, with a K of 5.1 mEq/L:
 |
| Normalized, with QRS of 92 ms. |
Cardiology deferred catheterization.
CK returned at 98000 IU/L.
She underwent emergent dialysis and fasciotomy.
Learning Point:
Hyperkalemia causes pathognomonic and completely recognizable ST elevation, especially in leads V1 and V2. It resembles Brugada pattern and is associated with Peaked T-waves and prolonged QRS.
Here is data from a post on use of beta-2 agonists to shift K into cells:
Terbutaline and Albuterol for Lowering of Plasma Postassium
–0.5 mg of IV albuterol reduces K by about 1.2 mEq/L.
— A 20 mg neb (most are 2.5 mg) lowers it by about 1.0 mEq/L.
–A 10 mg neb lowers it by about 0.6 mEq/L.
I give 0.25 mg of IM terbutaline to an adult, but only if it is critical, and add nebulized albuterol also. I’ve never given it IV, as I’m a bit reluctant to risk the cardiac irritability.
Here is a comprehensive blog post on this topic.
Here is a similar case caused by acidosis and cocaine toxicity.