This was submitted by Michael Fischer, one of our outstanding 2nd year EM residents at Hennepin Healthcare.
Case
A previously healthy female in her 40s presented 1 hour after abrupt onset 10/10
crushing chest pain that started while brushing her hair that morning.
The pain radiated to her bilateral jaw and right shoulder, and did not
seem to be exertional or pleuritic in nature.
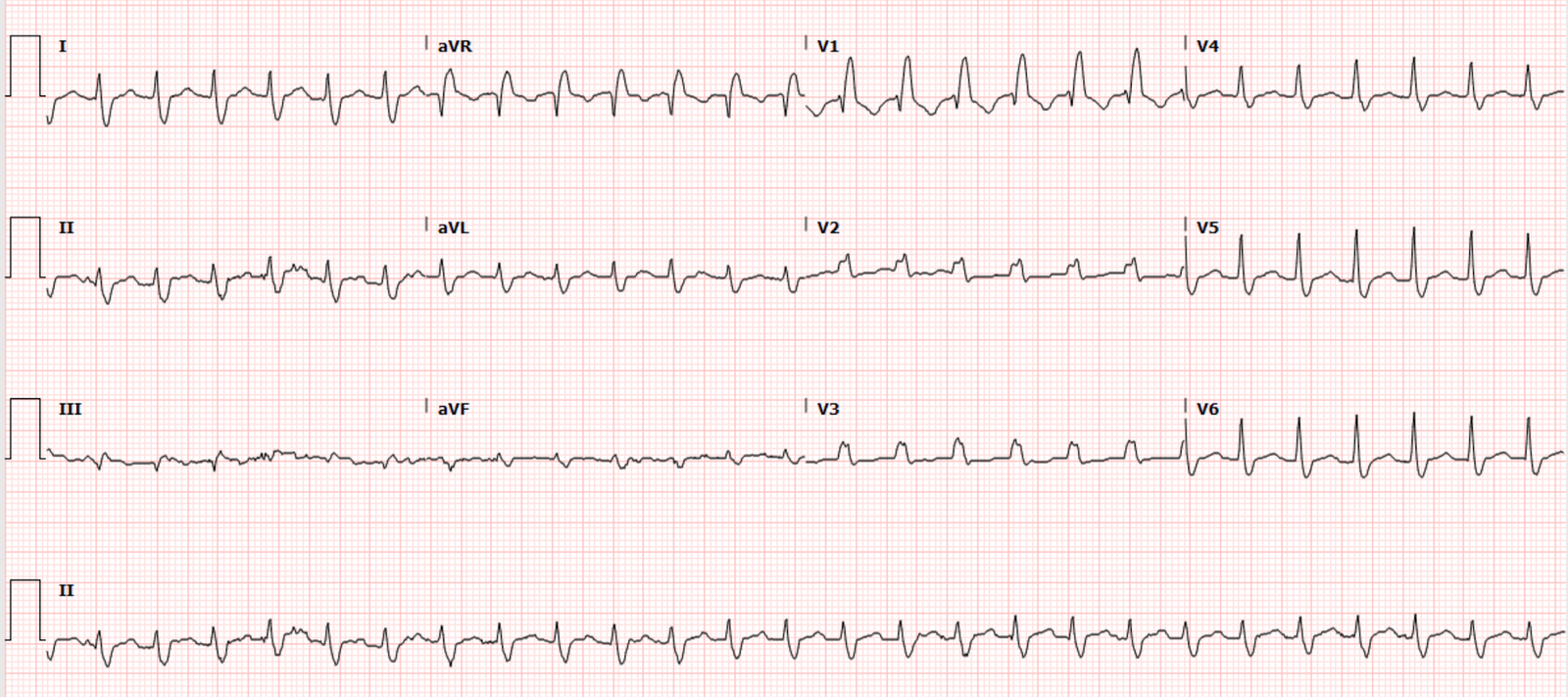
Here is her pre-hospital ECG:

What do you think?
Smith: V2 and V3 have some minimal ST depression with downsloping. This is highly suggestive of posterior MI.
This was read by EMS as non-specific. Aspirin 324mg was given by EMS.
Nitroglycerin spray x3 was also given which brought her pain down to 3/10
upon arrival to the ED. She was vitally stable with systolic BP of 140s.
No cardiac history, not taking any medications,
but does have 1st degree relatives with CAD.
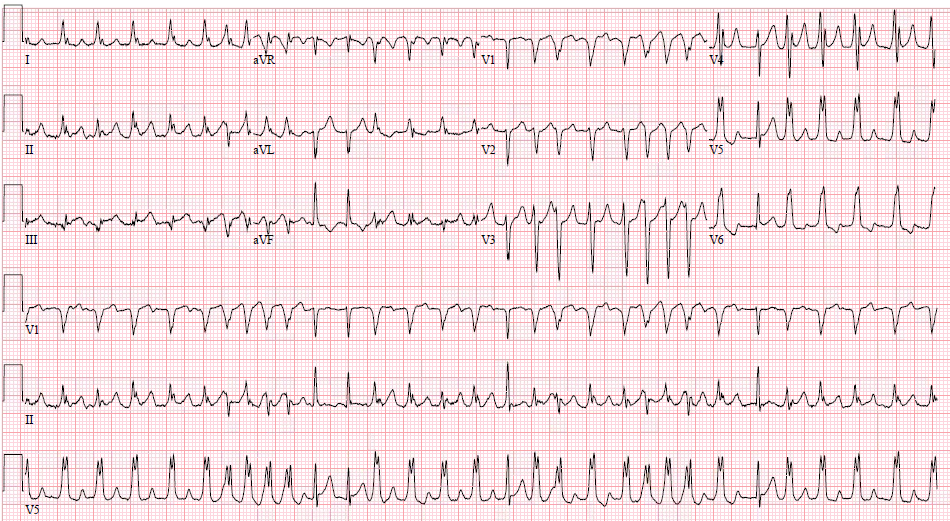
Here is her first ED ECG:

The ST Depression is more pronounced, and has extended to V4
This was interpreted as ST-depression in V2-V4. Additional sublingual
nitro was given x2, bringing her pain to 0/10 in her chest, however she
still had pain in her jaw.
Given the abrupt onset of pain, aortic pathology was also a concern.
Bedside echocardiography revealed grossly intact left ventricular
function, non-dilated aortic root. Suprasternal view of the aorta
revealed normal caliber aorta with no obvious dissection
flap. Upper extremity pulses were equal. D-dimer was sent as further
rule out for dissection.
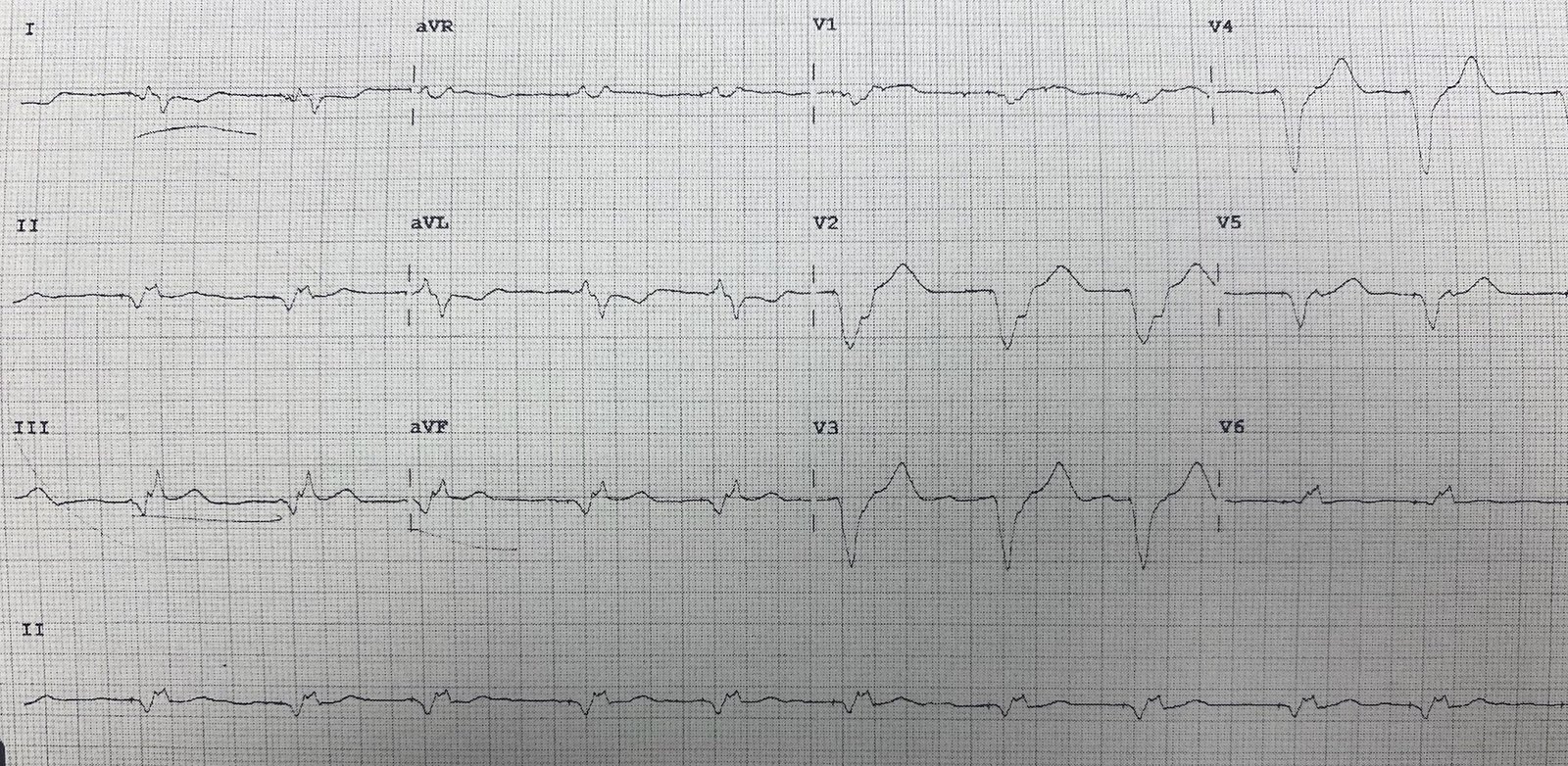
A repeat ECG was obtained with her chest pain resolved after nitroglycerin:

Almost completely resolved
This was interpreted as resolved anterior ST-depression.
Over the course of the next 30 minutes while labs were pending, her
chest pain slowly returned. Her troponin returned at 0.682 ng/mL (upper reference limit of
0.045 ng/mL), D-dimer negative. At this point, interventional cardiology was
consulted and recommended medical management with
plan for the catheterization lab that afternoon. She remained vitally
stable with systolic BP in the 130-140s. She was started on a nitro drip
and was heparinized.
Her chest pain continued to wax and wane on the nitro infusion. She
additionally received hydromorphone and ondansetron. Interventional cardiology was
consulted again regarding her waxing and waning pain, at which time
they took the patient to the catheterization lab.
Given her rapid improvement on nitro, it was thought that her symptoms
could be due to coronary vasospasm given her overall lack of CAD risk
factors. Ruptured plaque and coronary dissection remained leading
differentials as well.
Angiogram report:
Normal coronary arteries.
Left ventriculogram demonstrated apical ballooning and hypercontractile base consistent with stress-induced cardiomyopathy.
Takotsubo Cardiomyopathy- The Great Imitator!
As previously discussed in this blog, Takostubo cardiomyopathy may
manifest as T-wave inversion or ST elevation that can mimic a STEMI.
This patient’s ECG with anterior ST depression is an atypical ECG
presentation in takotsubo, and diagnostic of posterior
MI, prompting angiography to rule out acute coronary occlusion.
On
chart review, there was no inciting stressor thought to precede her
symptoms. She did well and was discharged on an ACE-inhibitor and
beta-blocker.
Smith comment: This ECG is very unusual for takotsubo. And although it correlates mostly closely with posterior transmural ischemia (posterior STEMI), it would not be unusual for subendocardial ischemia due to LAD spasm or LAD subtotal thrombosis. Thus, I am not entirely convinced of takotsubo in this case.
All management was appropriate. The cath lab certainly needed activation. The coronaries were clean. There was apical ballooning on ventriculogram.
However, the cath report does not mention whether the LAD wraps around to the inferior wall, and there was no intravascular ultrasound (IVUS) to prove absence of ruptured plaque that does not manifest on plain angiogram (which only shows the lumen of the artery and, unlike IVUS, does not show extraluminal plaque).
Moreover, the onset of chest pain was without inciting event, as usually happens with takotsubo, and was relieved with nitroglycerin, which strongly suggests some element of coronary ischemia.
Thus, we may never know whether this was LAD ACS, LAD spasm, or a very strange sort of takotsubo.