One of my residency grads sent this.
A male in his 50’s with h/o CAD presented with 2 days stuttering chest pain (also with nausea, diaphoresis, and SOB). The chest pain had been constant for 2 hours.
“His first ECG was reviewed by a partner [who has not had as much training in ECGs) who said it was ok for the patient to wait in triage. When he was roomed I took a look at his initial ECG.”
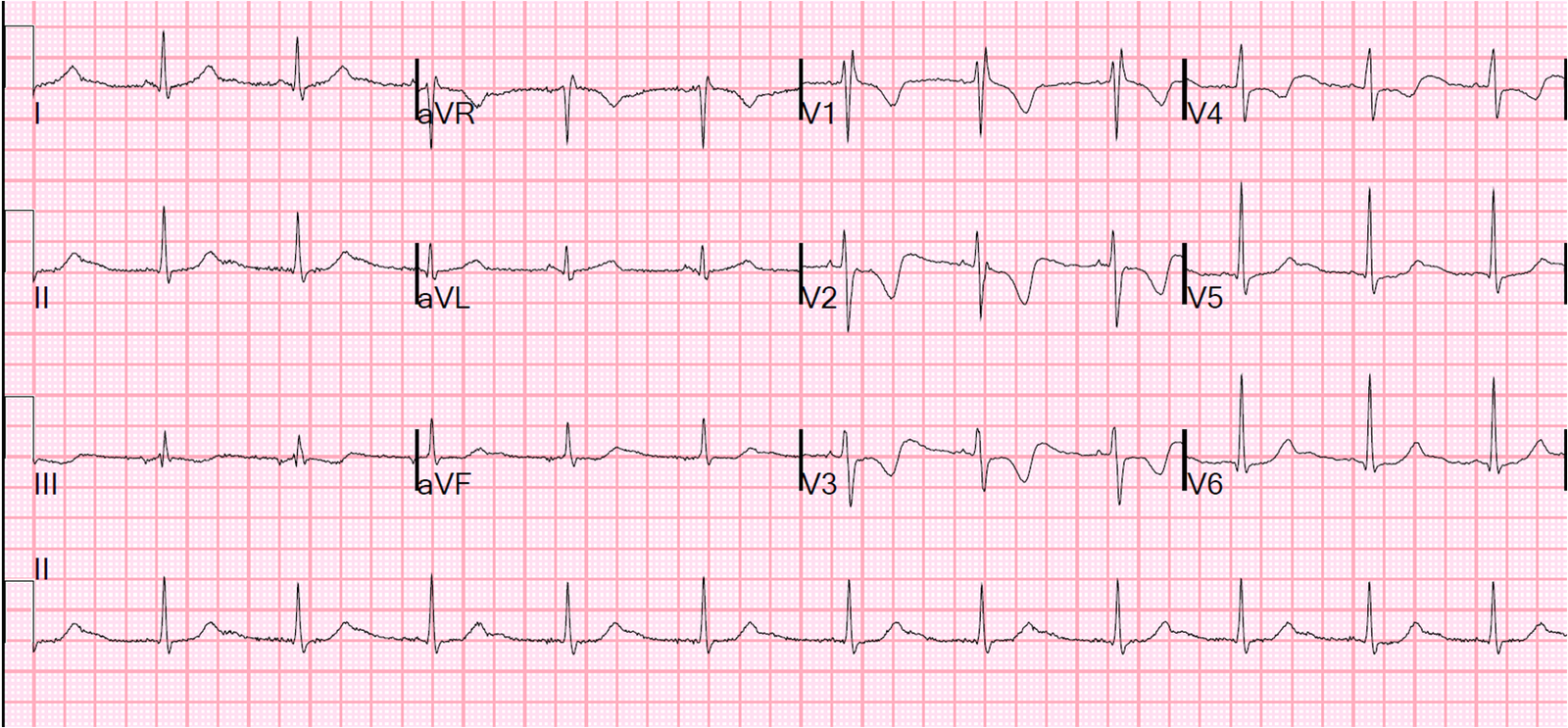
Here it is:
 |
| This was his assessment: “I saw the T-wave in inferior leads and immediately ‘freaked out.’ Then I saw the subtle but non diagnostic ST elevation, but mostly it was the look of aVL which I’ve heard you talk about a million times now as being specific for inferior ischemia.” |
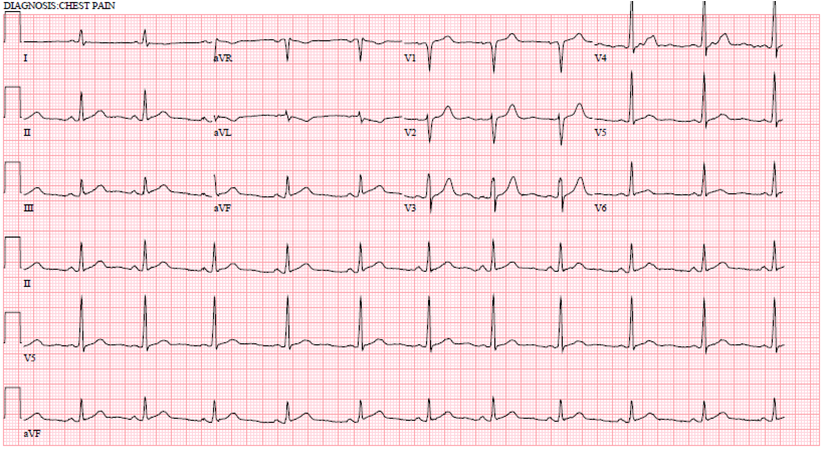
He got a repeat right away (24 minutes after the first):
 |
| “This showed STEMI, so I activated the cath lab.” |
Outcome:
The patient had severe diffuse CAD with a 99% thrombotic stenosis culprit in the circumflex, with TIMI-1 (very slow inadequate) flow. It was stented.
Peak troponin was 53.5 ng/mL.
He is scheduled for CABG in 2 weeks.
What is the outcome of patients with MI who present with subtle ST elevation?
Is it more benign than those with diagnostic ST Elevation?
The authors have a very aggressive policy of taking patients to the cath lab immediately even for low suspicion of STEMI. They studied 504 consecutive patients who were taken to the cath lab for suspicion of coronary occlusion. 86% were found to have TIMI 0 or 1 flow. 18% of these patients did not have any lead with at least 1 mm of ST elevation measured at the J-point. These patients more frequently had multivessel disease and longer delays to reperfusion. They had the same incidence of subsequent death or re-infarction.
Their study underestimates the number of subtle STEMI because they used 1 mm even in V2 and V3. The guideline recommended cutoff for these leads is 1.5 mm for women, 2.0 mm for men age greater than 40, and 2.5 mm for men aged less than 40.
Their conclusion was: “Subtle STEMI is frequent in clinical practice and is usually associated with acute total coronary occlusion. Therefore, it should be diagnnosed and treated in the same expeditious manner as marked STEMI. (Marti D et al. Incidence, angiographic features, and outcomes of patient presenting withsubtle ST-elevation myocardial infarction. Am Heart J 2014; 168:884-90.)
Learning point:
It is important to recognize subtle ST elevation myocardial infarction. These patients are frequently not recognized and not taken for cath until the following day. This study shows that patients with coronary occlusion frequently have minimal ST elevation.