This Case was sent by Atif Farooqi and Scott Weingart, from Stony Brook.
This is a 70-something with history of CABG who presented with 30 minutes of SOB and palpitations.
Here is his ECG:
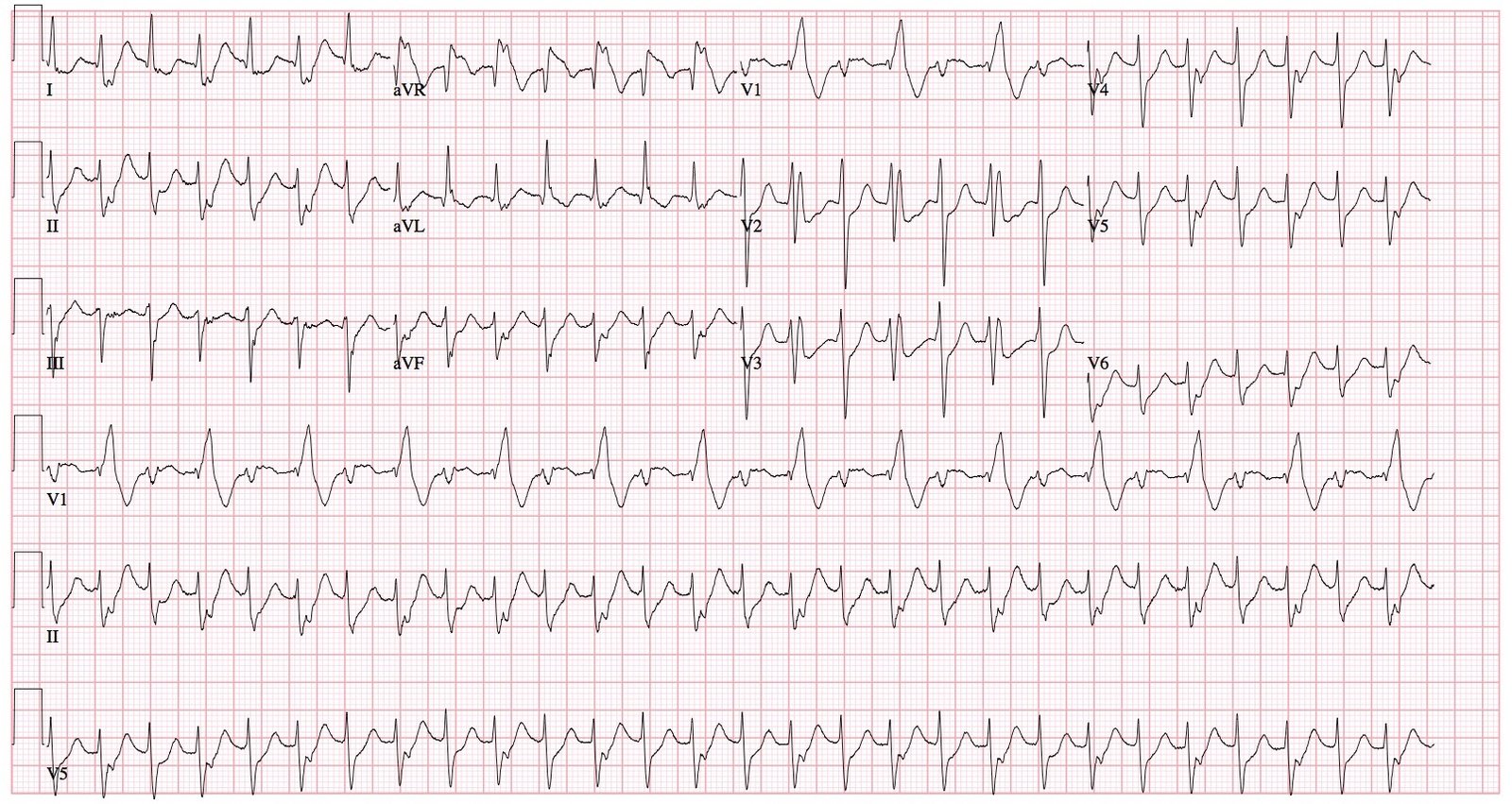 |
| What is it? |
Atif wrote this:
“My first thought was perhaps a bidirectional V Tach, though the pt is not on digoxin and otherwise has no discernable reason to be in BVT. Scott was considering maybe an intermittent aberrant conduction, though we thought it odd for it to be strictly alternating beats.
Here is my answer:
Atif,
Interesting EKG!
I think it is SVT with every-other-beat-aberrancy.
–Every QRS comes right on time, perfectly regular, so it can’t be Bigeminy.
–Every
other beat is RBBB, which is the most common type of aberrancy because
the right bundle has a longer refractory period than the left.
–The inbetween beats are of normal duration (100 ms). The axis does not alternate. There is no alternating RBBB and LBBB. So it can’t be bidirectional tachycardia (neither bidirectional VT nor bidirectional SVT).
–There are no P-waves.
So this is AVNRT with alternating aberrancy (Scott was right!).
Additionally, both the aberrant and the normally conducted beats have significant ST depression.
Bidirectional Tachycardia implies alternating frontal plane axis, from -60 to +120, or alternating LBBB and RBBB.
Bidirectional tachycardia can be Bidirectional Ventricular Tachycardia, as with Digoxin toxicity. The etiology may be:
1. alternating location of origin of the VT ectopic focus, or
2. alternating routes of depolarization from a single ectopic focus
Bidirectional VT may also result from aconite toxicity, as in this case I reported, which has alternating RBBB and LBBB.
Bidirectional Tachycardia can alternatively be due to SVT with Bidirectional Aberrancy: the aberrancy may be due to:
1. RBBB with alternating LAFB (left axis) and LPFB (right axis), or
2. Alternating RBBB and LBBB.
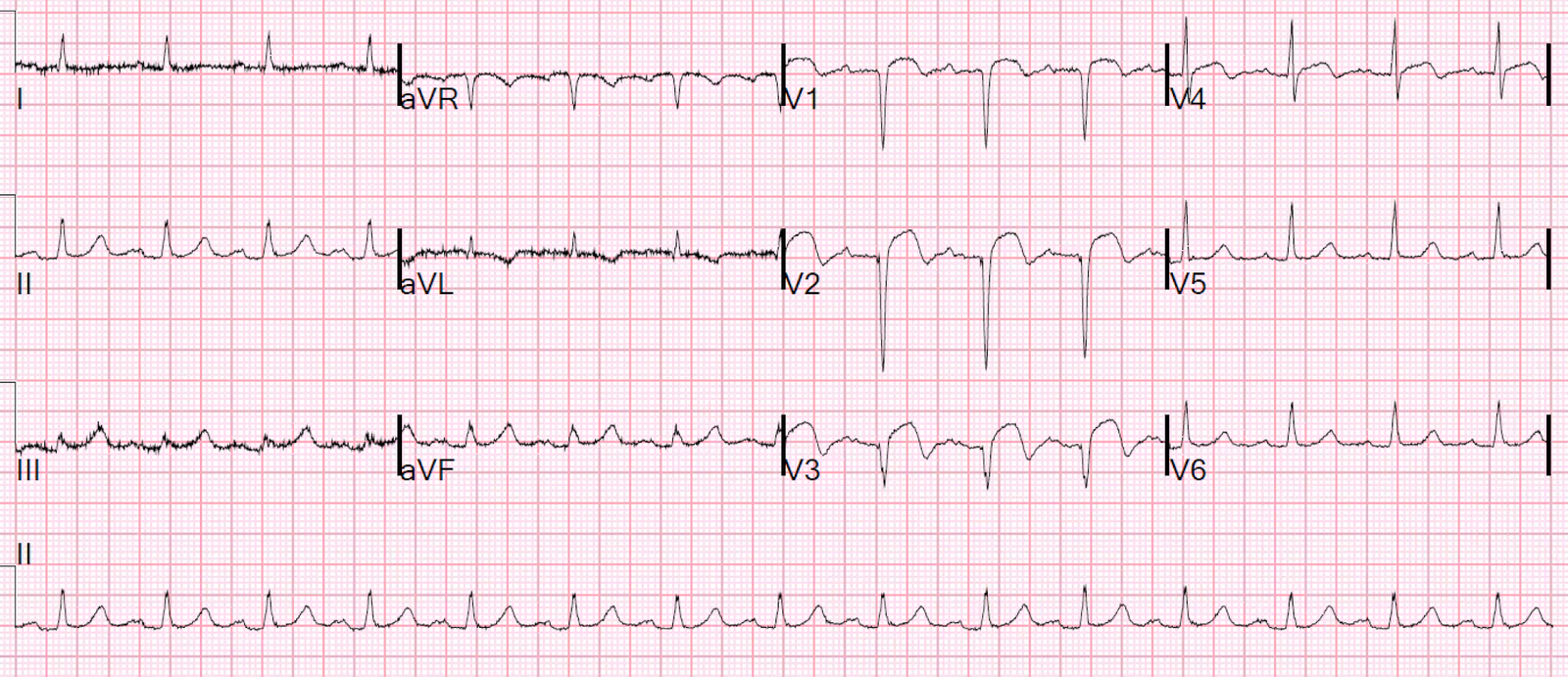
Here is the ECG from this case of Aconite Toxicity:
 |
| Alternating RBBB and LBBB. Intervals are regular. |
This case presented here today does NOT have alternating frontal plane axis, nor does it have alternating RBBB and LBBB, so is not bidirectional tachycardia.
Case continued:
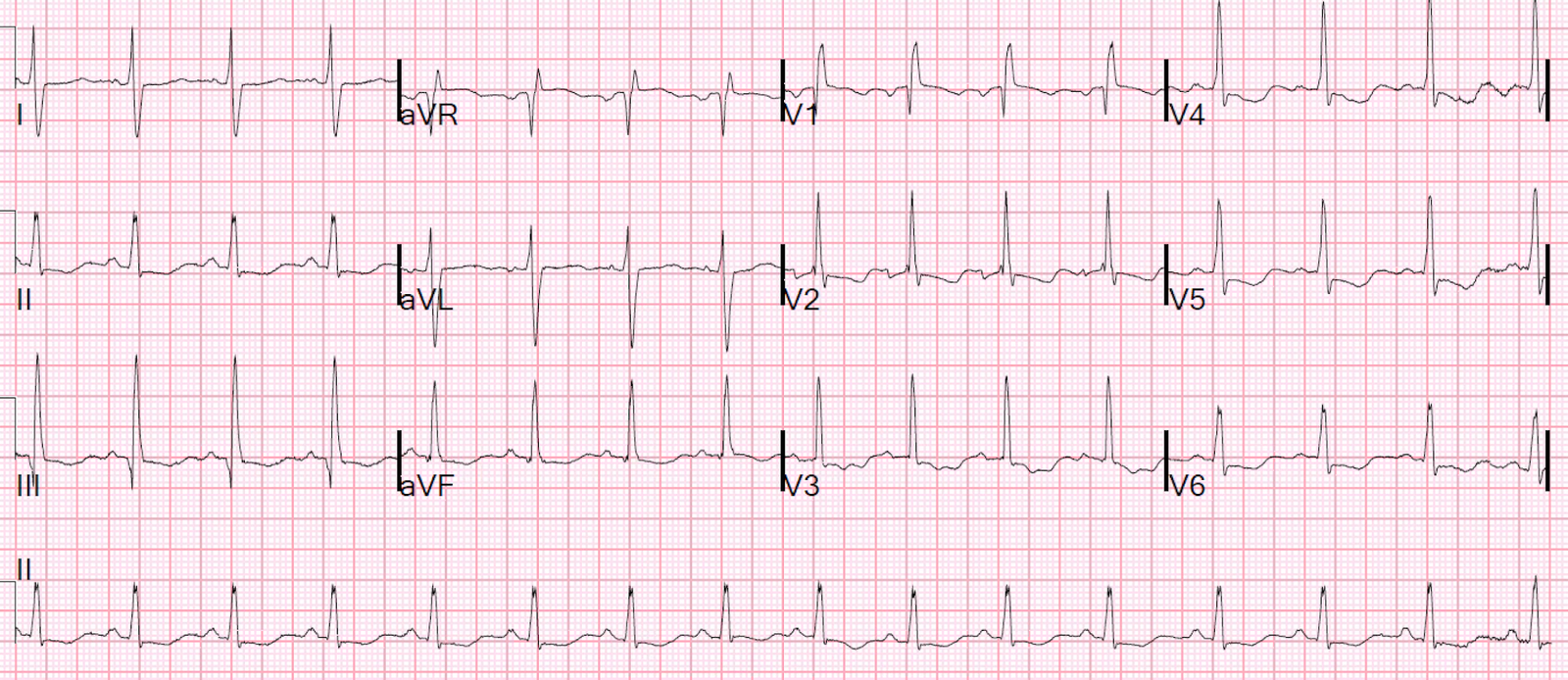
The attending gave IV Metoprolol, (the patient was supposed to be taking oral metoprolol as an outpatient), and the rhythm changed to the following:
 |
| This appears to be sinus, though the P-waves are not obvious. This subsequent ECG proves that the first was SVT with aberrancy: the complexes are identical to the non-RBBB beats of the first ECG. There is also persistent ST depression. Hopefully now that there is no longer tachycardia, this ischemia will resolve. It is typical for metoprolol to convert an AVNRT. I would have tried adenosine. |