===================================
MY Comment by KEN GRAUER, MD (11/19/2020):
===================================
I’d like to revisit one of Dr. Smith’s ECG Blog posts from 2012 for 2 Reasons:
- Reason #1: It highlights the challenge of assessing anterior ST elevation in a certain type of patient.
- Reason #2: There is one more easy-to-overlook but important finding on the ECG that was not initially detected.
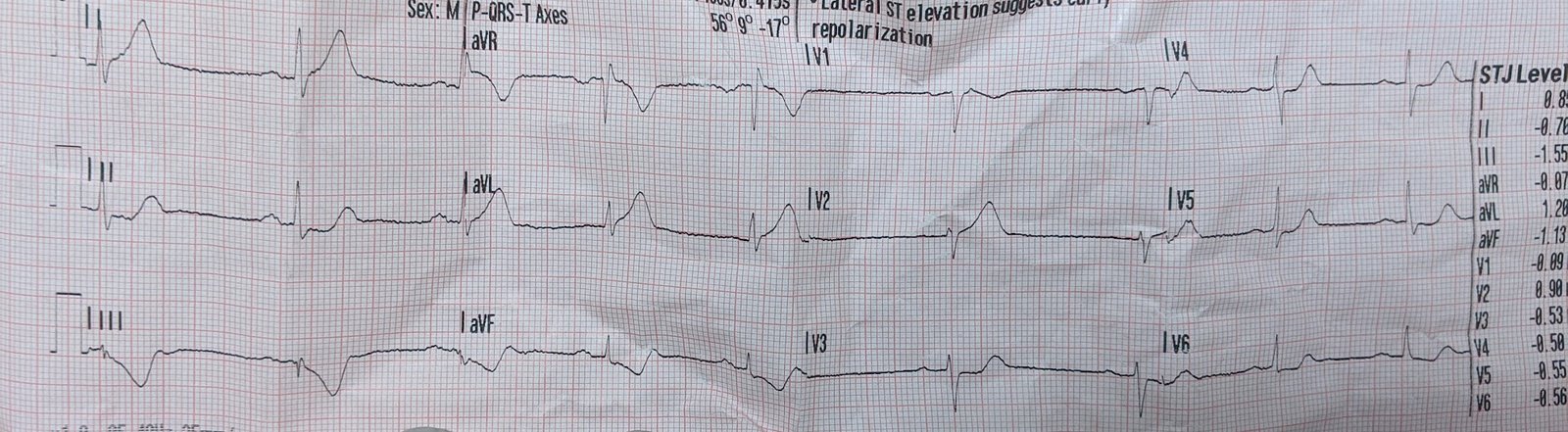
TAKE a LOOK at the ECG in Figure-1. This is the initial tracing from this patient who presented to the ED with new chest pain and dyspnea.
- There is ST elevation in leads V1-thru-V3 of ECG #1, attaining 3-4 of J-point ST elevation in lead V3.
- QUESTION #1: Given the history (ie, new-onset chest pain) — Should the cath lab be activated? IF not — WHY not?
- QUESTION #2: What other important finding in the limb leads should be recognized?
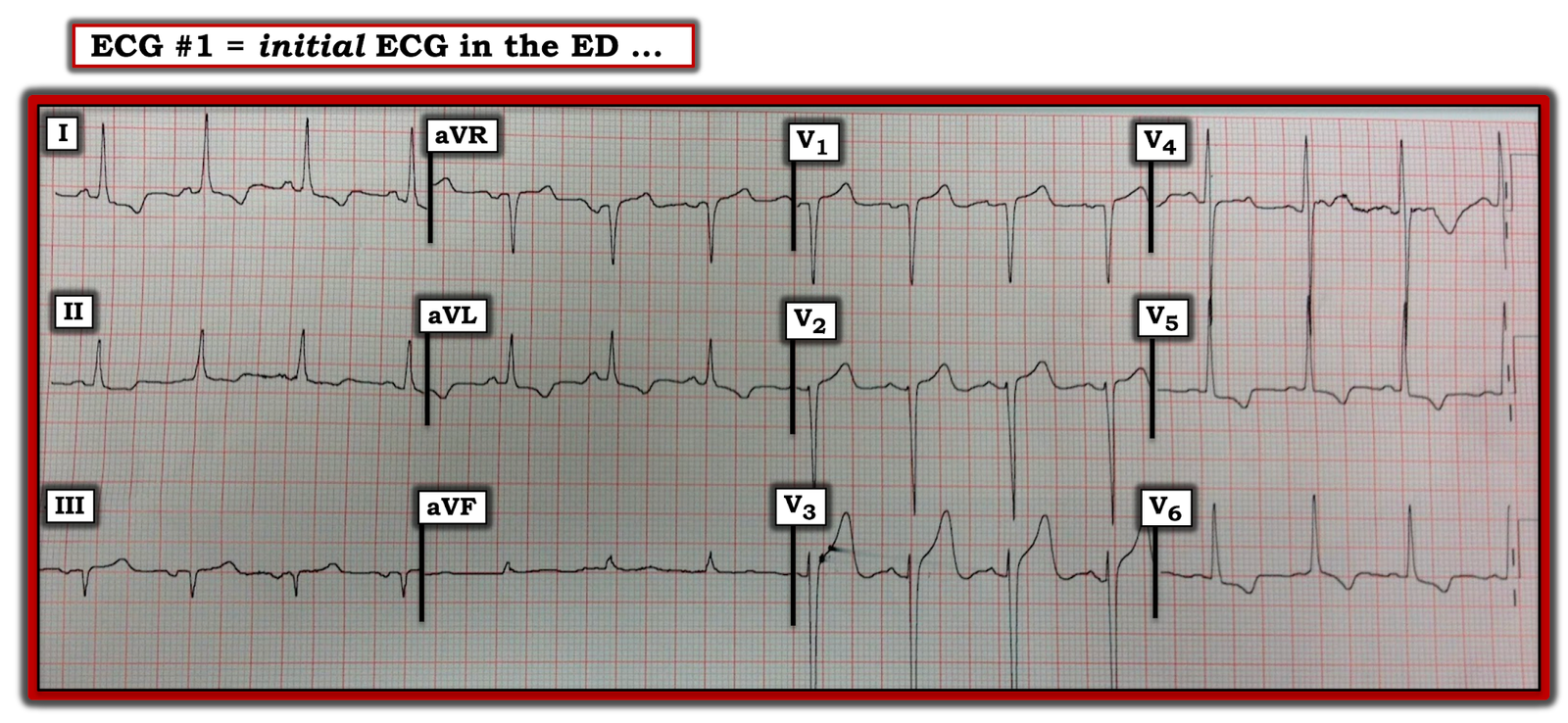
Figure-1: The initial ECG in the case from our February 8, 2012 post in Dr. Smith’s ECG Blog (See text).
ANSWER to QUESTION #1: As discussed by Dr. Smith back in 2012 (and reinforced many times in the 8 years since on this Blog) — the reason not to activate the cath lab based on the ECG shown in Figure-1 — is that this ECG is almost literally screaming, “The patient has LVH!”
- QRS amplitude is dramatically increased in virtually all chest leads in ECG #1 (ie, the S in lead V2 ~23 mm; the S in lead V3 is well over 20 mm [cut off at the bottom of the paper]; the S in lead V4 ~21 mm; the R in lead V5 ~15 mm). As per the Table in Figure 3 (that I have placed in the Addendum below) — multiple voltage criteria for LVH are satisfied in ECG #1.
- In addition — both anterior and lateral leads in ECG #1 manifest ST-T wave changes typical for LV “Strain”. Among many discussions in this Blog about the “anterior lead STEMI-mimic” of LVH — the June 20, 2020 post probably illustrates this phenomenon best. In My Comment (at the bottom of the page at this June 20, 2020 link) — I illustrate how the mirror-image of anterior ST elevation may simulate the depressed ST-T wave seen in lateral leads when there is LV “strain”. As a result — the anterior ST elevation and increased QRS amplitudes seen in ECG #1 are both features in the unifying diagnosis of LVH with LV “Strain”.
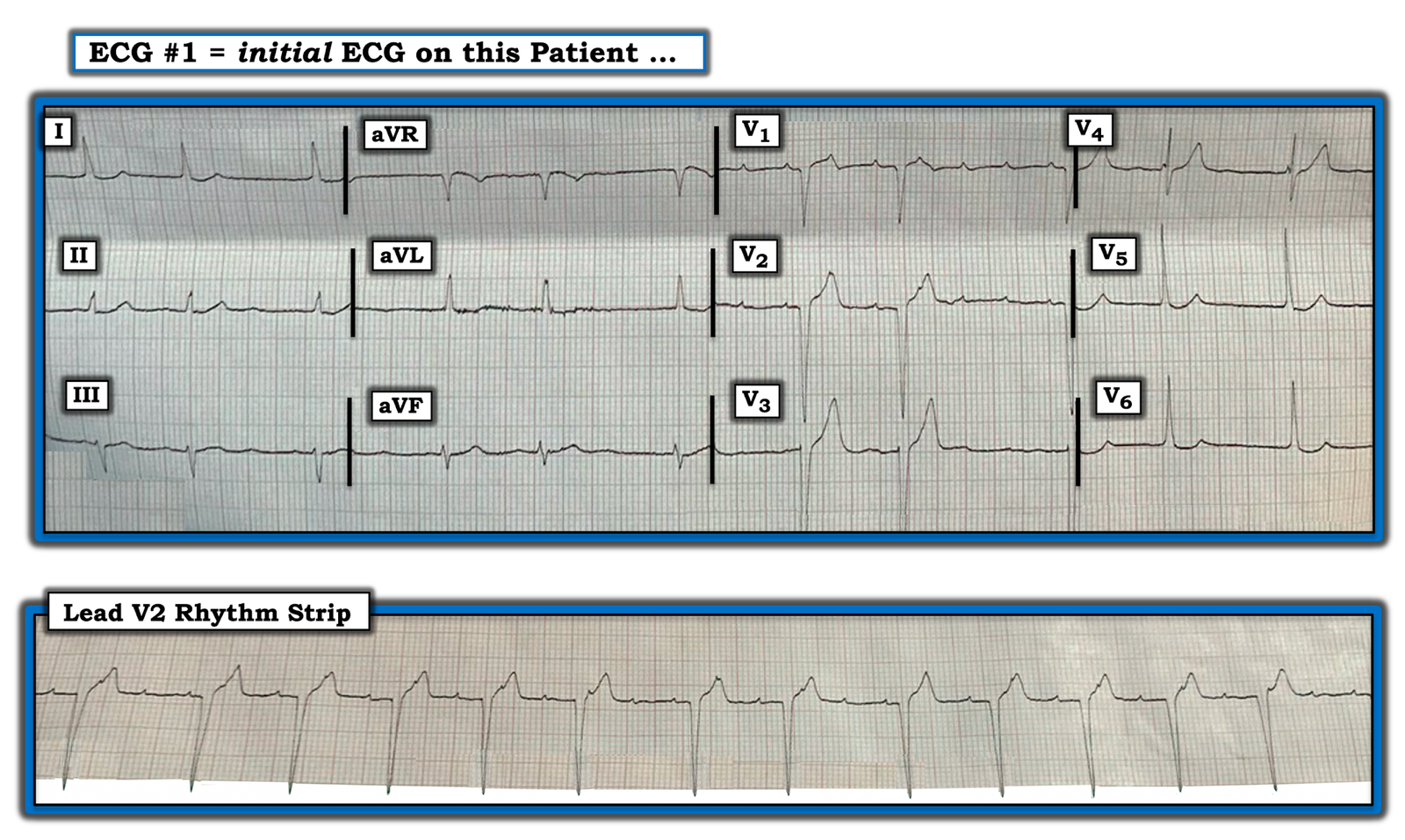
Final QUESTION: Did you notice in ECG #1 that the P wave in lead I is taller than the P wave in lead II?
- WHY might this be so?
ANSWER to QUESTION #2: The reason the P wave in lead I of ECG #1 is taller than the P wave in lead II (and also the reason why the P wave and QRS complex in lead III in ECG #1 are both negative) — is that there is LA-LL Lead Reversal!
- My favorite on-line “Quick GO-TO” reference for the most common types of lead misplacement comes from LITFL ( = Life-In-The-Fast-Lane). Simply put in, “LITFL Lead Reversal” into the Search bar of your internet browser — and the link comes up instantly!
- In Figure-2 — I have put the initial ECG = ECG #1 on the TOP, with addition below it of a box listing the effects that LA-LL Lead Reversal has on the ECG.
- In the BOTTOM of Figure-2 — I have inverted lead III — switched the position of leads I and II — switched position of leads aVL and aVF — and left aVR alone. I have labeled this new tracing as ECG #2 — and have placed this under the initial ECG — so that we can compare how correcting for the effects of LA-LL Lead Reversal would result in an ECG that would look like ECG #2. Therefore — Although clinical management in this case would not have been changed (because our interpretation of this patient’s ECG would still have been marked LVH and not acute anterior OMI) — Comparison of ECGs #1 and #2 tells us how much limb lead appearance would have changed IF all limb leads had initially been correctly placed.
- NOTE: For another example of LA-LL Lead Reversal — Please see our August 28, 2020 post.

Figure-2: Showing the effects of LA-LL Lead Reversal — then taking another look at ECG #1! (See text — and See LITFL Lead Reversal).
LEARNING Points from this Case:
- Some types of lead misplacement are obvious. Others (such as the LA-LL lead reversal in today’s case) can be ever-so-easy to overlook. The “tipoff” to LA-LL reversal in ECG #1 — is that the P wave in lead I is clearly larger than the P wave in lead II (and that is unusual when there is sinus rhythm).
- Additional “tipoffs” that something may be amiss — include the negative P wave and negative QRS complex in lead III that can be seen, but which are not overly common (especially when seen in association with a P wave in lead I that is taller than the P wave in lead II).
- Finally — Remember that marked LVH with overly deep anterior lead S waves may be accompanied by a surprising amount of anterior ST elevation which is usually not indicative of anterior OMI, but rather a mirror-image of LV “strain” as seen in anterior leads.
ADDENDUM: Criteria I favor for the ECG diagnosis of LVH.
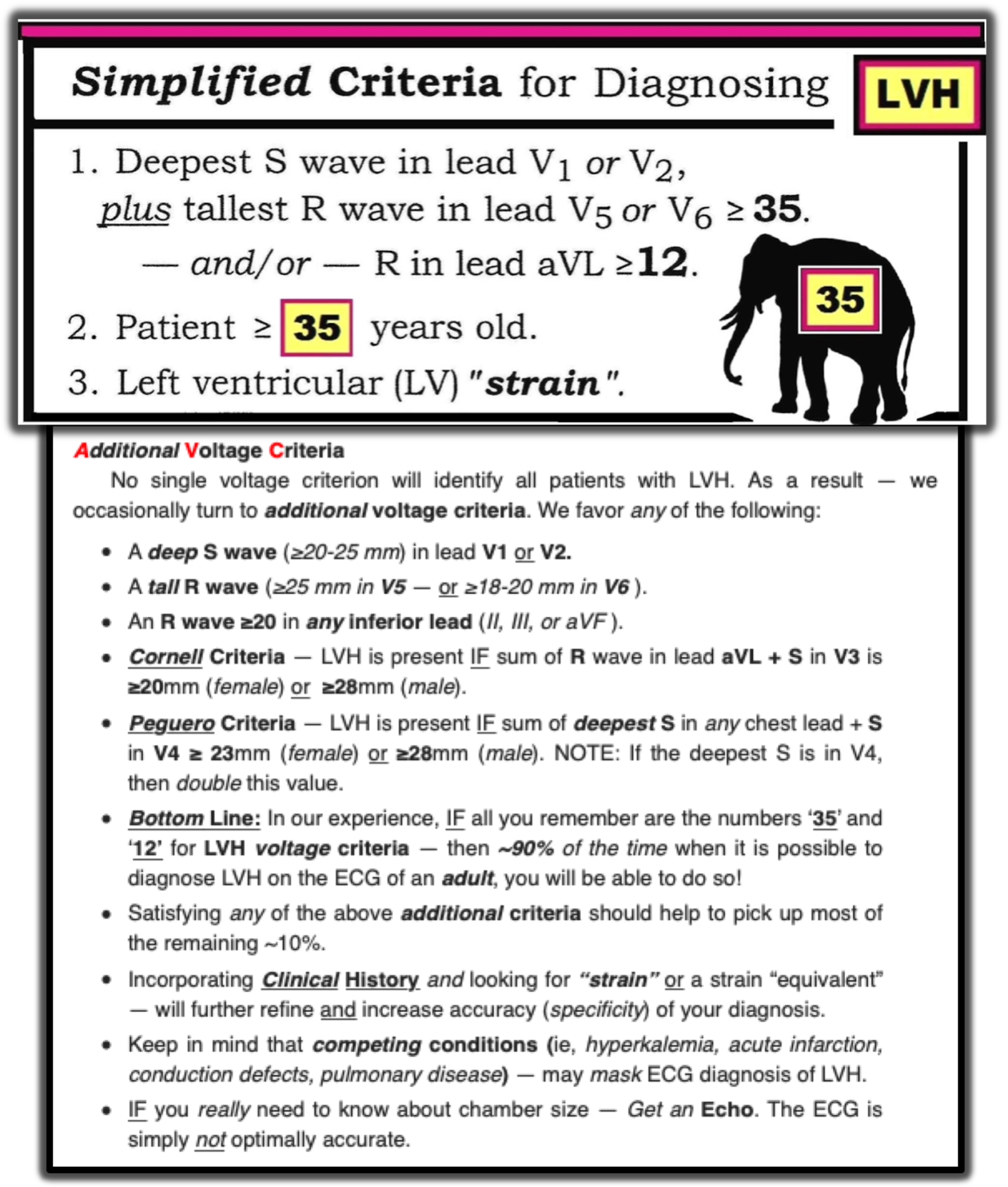
Figure-3: Criteria I favor for the ECG diagnosis of LVH (This figure excerpted from My Comment in the June 20, 2020 post of Dr. Smith’s ECG Blog). Note that a number of voltage criteria listed here are satisfied in ECG #1.
================
NOTE: My sincere THANKS to Anderson Santos (from Brazil) for catching this subtle example of lead misplacement!
================