Case 1
This case was sent by Michael Masias (EMCurious, Twitter handle: @EMedCurious), an ultrasound fellow in the Department of Emergency Medicine at UC San Diego.
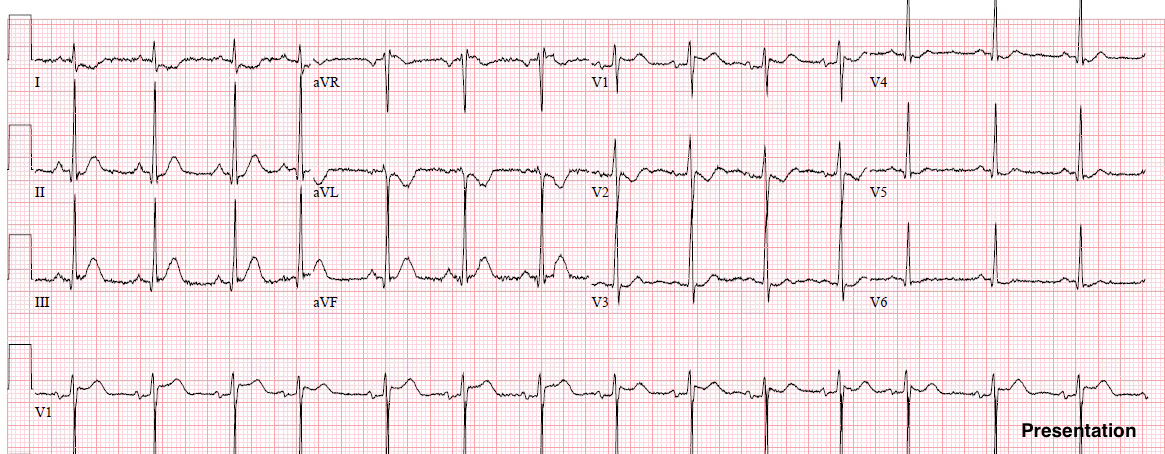
He sent this ECG with the following inquiry:
“What do you think about this? 21 year old with chest pain. I am getting a result of “STEMI” by using the 3-variable formula, and “no STEMI” with the 4-variable.”
 |
| Computerized QTc = 418
Here was my immediate answer:
I should also have added that tachycardia does not fit with anterior MI unless there is cardiogenic shock. More Analysis: There is ST Elevation in V2-V5 that meets “criteria” for anterior STEMI. There is over 3 mm of STE (at J-point, relative to PQ jct.) in V3 and V4.
In a 21 year-old, only 2.5 mm in V2 and V3 is required, and only 1 mm in V4. So there are 2 consecutive leads with STE that exceeds “critieria.” 3-variable formula = 24.56 (above 23.4, indicating LAD occlusion) 4-variable formula = 12.96 (very low due to high QRS voltage in V2) Remember:
This formula is meant to help differentiate early repol from LAD occlusion.
It does not differentiate other etiologies of STE elevation!
The 4-variable formula is more accurate, but this is not validated. More information: “21 year old with 3 days of sharp left sided chest pain. He had a pharyngitis 1.5 weeks prior. He was transferred to me for STEMI but when he arrived he was very comfortable and the tachycardia didn’t fit, in my opinion. So I did a bedside echo and he was hyperdynamic with no signs of heart failure, and all walls looked good to me. I did speak with the interventionalist on call and they thought it was early repol.”
Smith comment: this was a very astute evaluation. Anterior MI will not have hyperdynamic cardiac function with excellent ejection fraction! |
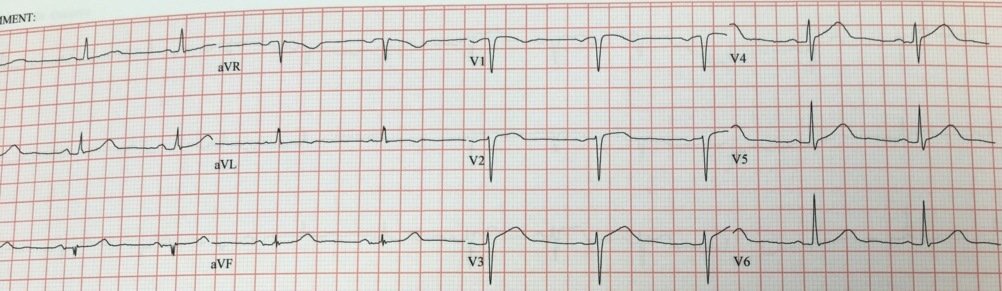
We recorded another ECG 45 minutes later:
 |
| There is less ST elevation now. |
“The first troponin I returned at 4 ng/mL. The patient remainded comfortable in the ED and cardiology just recommended observation so I admitted him for formal echo and serial troponins.”
“The patient never underwent angiogram, but echo did not show a wall motion abnormality and this rules out STEMI.”
Case 2
Medics came into the ED and showed me this prehospital ECG on a 40-something patient with chest pain:
 |
| My opinion was that this was normal ST Elevation, not LAD occlusion.
There is ST Elevation in V2-V5. The STE meets STEMI criteria. |
Why do I think it is not STEMI?
Because the ST elevation is more pronounced than the T-wave is hyperacute (low T/ST ratio). The ST segment is either downsloping (saddleback) or almost flat. This ST segment shape is a result of the relatively low T-wave voltage. When a T-wave is tall and large (not this case), the ST segment by necessity slopes steeply upward to the tall T-wave. When a T-wave has comparatively low voltage, as do these T-waves, the ST segment is relatively flat.
I went to talk with the patient. He had been having a cough and fever for about a week, and had gone to a clinic for dyspnea 3 days prior. The pain had been intermittent for the previous 3 days and there seemed to be some positional component to it, but he really could not describe it well and was holding his chest.
We recorded this ED ECG:
 |
| Approximately the same. |
I was not convinced, even by my formulas. We sent a troponin I, which returned quite elevated, at 4.80 ng/mL, within an hour of arrival.
That caught my attention, but I thought, due to the symptoms and the ECG, that this was probably myocarditis.
I repeated the ECG:
 |
| Not much different |
I did a bedside echo and was worried for an anterior wall motion abnormality (WMA).
Unfortunately, this is common in myocarditis. Absence of WMA would confirm myocarditis. Presence of WMA does not differentiate.
However, I was not willing to bet the patient’s life on it. I talked with the interventionalist and we arranged for the patient to go to the cath lab, but did not actually “activate” the cath lab as one would with a STEMI.
A repeat troponin was 4.9 ng/mL
The coronaries were clean.
Next day formal contrast echo was normal.
Diagnosis: myocarditis.
Next day, a friend at another hospital found a previous ECG on this patient:
 |
| The same kind of ST elevation was not present previously. This shows that the findings were NOT due to early repol, but a consequence of myocarditis. |