A middle-aged patient presented feeling moderately ill. He had an ECG recorded.
 |
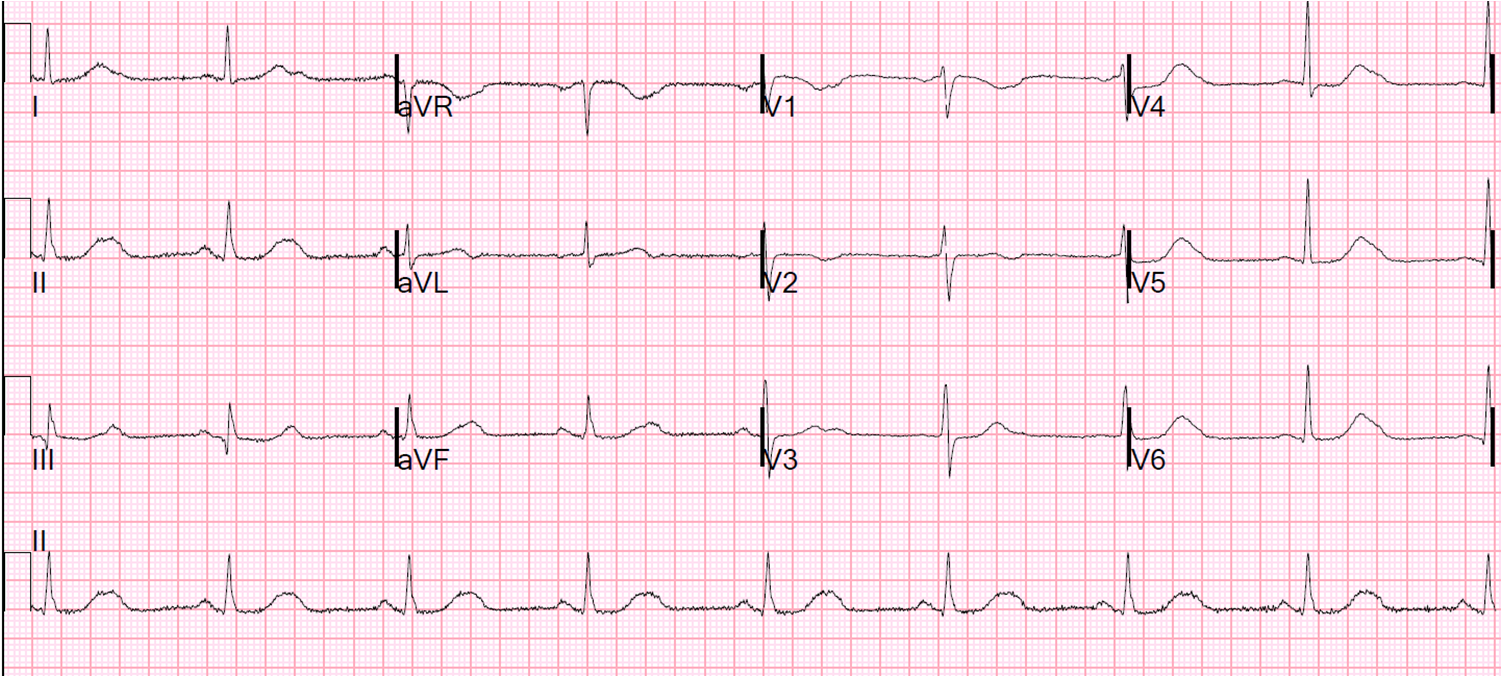
| QRS 102 ms. There are peaked T-waves. See V4 especially. The ST segment is horizontal until it abruptly rises to a very peaked T-wave. The T-wave is “tented” to a point. It is all but pathognomonic for hyperkalemia. |
By history, the patient had no reason to have hyperK on history. A recent previous ECG, done at a K of 4.5 mEq/L, was sought by the residents:
 |
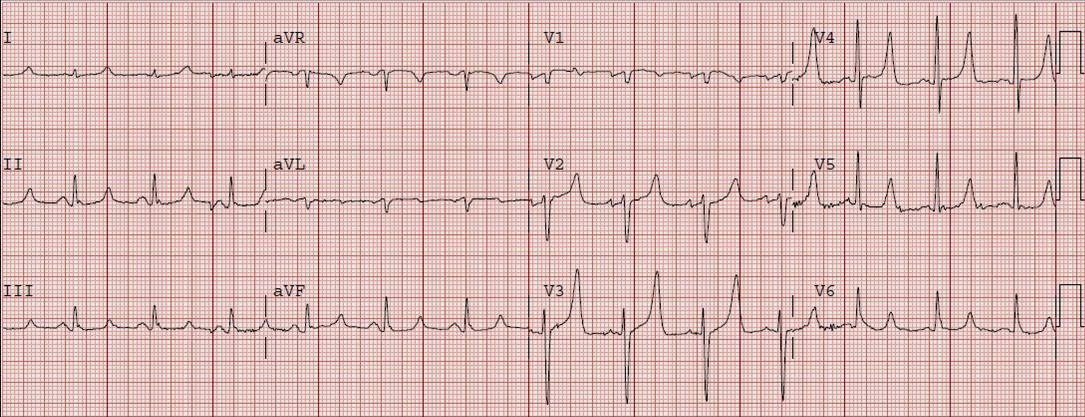
| The old ECG also shows very peaked T-waves. The residents concluded that these were his baseline T-waves. Were they correct? |
No! Notice the ST segments in the ECG at presentation are much more flat, and they then rise much more quickly to a peaked T-wave, especially in lead V4.
Case Conclusion
Residents had already made the comparison and decided that it was not different. Several minutes later, I saw these two ECGs and immediately saw the difference. I could see that the new ECG was diagnostic of hyperkalemia, and told the residents that they must immediately start treatment. As we were walking to his room, and before Calcium could be given, the patient had a v fib arrest while in his room, before his K returned from the lab. This was a presumed hyperkalemic arrest. He was immediately defibrillated and given Calcium. His K returned at 7.0 mEq/L.
Some say you don’t need to treat hyperK unless there is QRS widening, claiming that merely having peaked T-waves is not enough. This is only one case, and anecdotal, but we found no other etiology of arrest in this patient. The patient had new renal failure as the etiology of hyperK.
1. Peaking of T-waves occurs in other conditions than hyperkalemia, such as early repolarization. Comparison with the previous ECG must be done very carefully
2. I always treat immediately if I think the ECG is affected by hyperK. I do not wait for the laboratory results