An elderly male with history of atrial fibrillation presented by ambulance. His prehospital tracing (lost, sorry) showed a 6-beat irregular run of wide complex tachycardia. The medics were worried about a run of ventricular tachycardia (VT).
Here is his first ED ECG:
 |
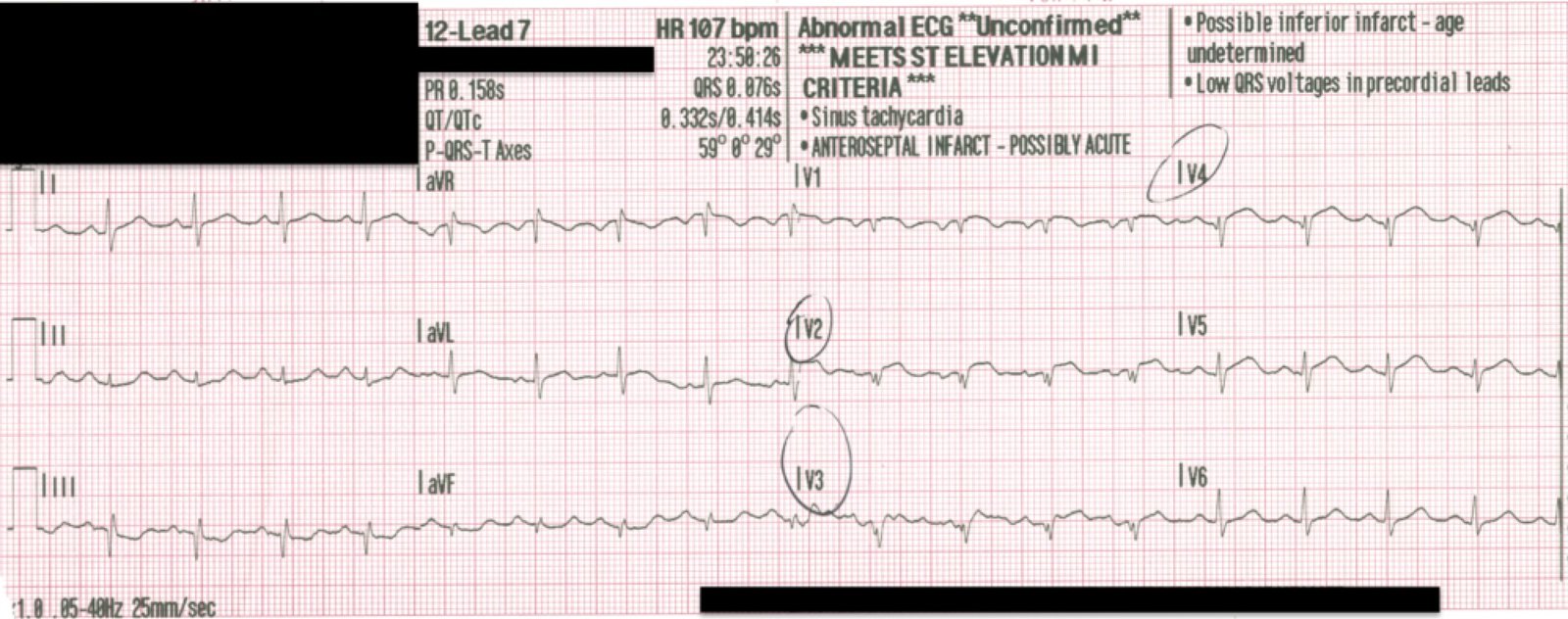
| There is an irregularly irregular rhythm with QRS duration of 115 ms. (There is also left axis deviation, probably left anterior fascicular block) This is atrial fibrillation. Notice there are three wide complex beats in lead II across the bottom. Are these PVCs? Was the 6 beat run due to VT? What is going on? |
Here is a magnification with annotation:
 |
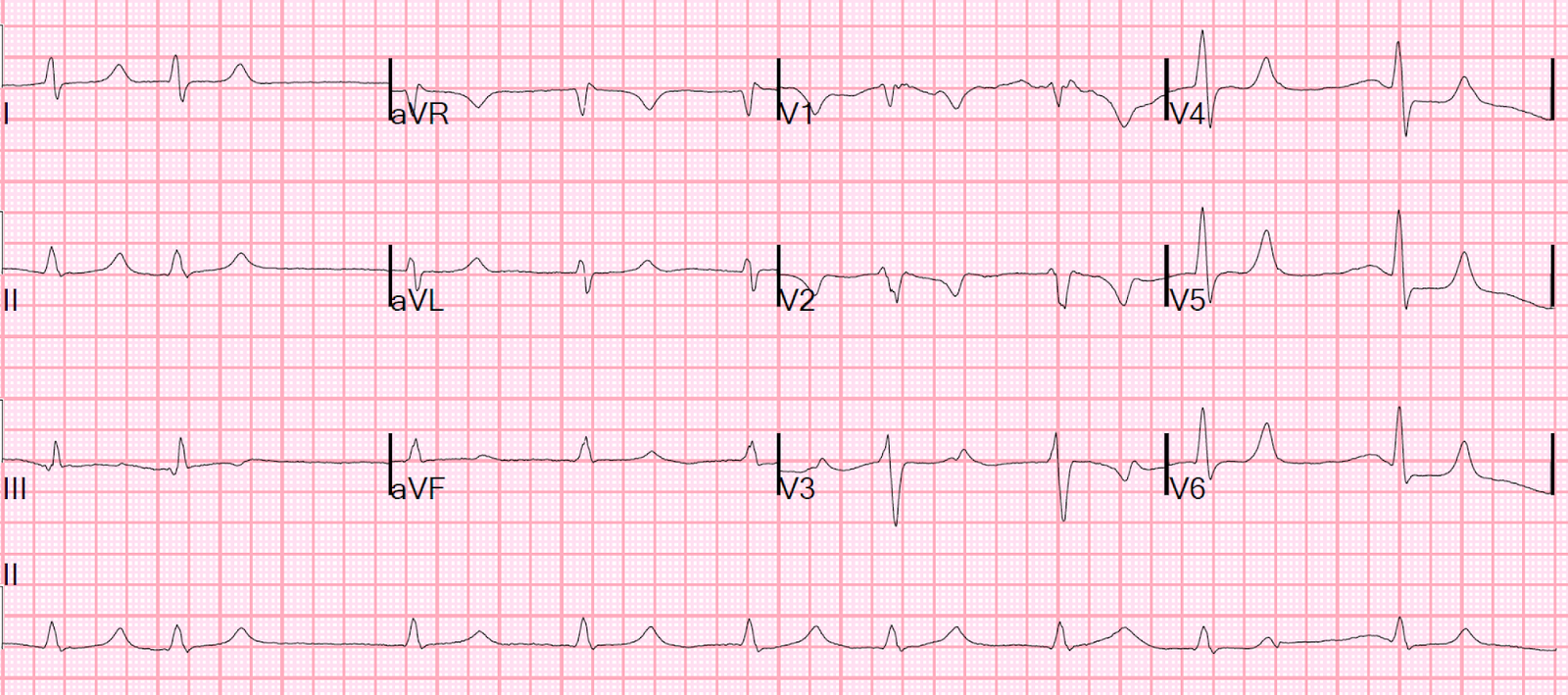
| First, notice that beats 8 and 14 (black arrows) are identical.
Second, notice that beat 14 is simultaneous with leads V1-V3, and that beat 14 in lead V1 has an RBBB pattern. The right bundle has a longer refractory period than the left bundle, so aberrancy is most likely to have an RBBB pattern. What is this aberrancy in atrial fibrillation called? Ashmann’s phenomenon. |
Ashmann’s Phenomenon: After a relatively long R-R interval, repolarization is delayed and there may be an aberrant beat if it comes relatively early. In Ashmann’s phenomenon, the AV node and HIS bundle have shorter refractory periods than the bundle branch, in this case the right bundle, and so the impulse traverses both the AV node and HIS bundle and then the left, but not right bundle branch.
The phenomenon is frequent with a long-short sequence:
Complex 8: The preceding R-R interval affects the refractory time of the subsequent beat.
Thus, the long R-R interval between complexes 6 and 7 (410 ms) makes the refractory period of complex 7 longer, then complex 8 comes early at 320 ms and thus complex 8 has aberrancy.
Complex 12: this is also wide, but I cannot measure a definite difference in QRS duration between it and complexes 8 and 14. The preceding R-R interval (between complexes 10 and 11) is again long, making the refractory period of complex 11 long, resulting in aberrancy in complex 12.
Complex 14: the long R-R interval between complexes 12 and 13 (560 ms) makes the refractory period of complex 13 longer and thus complex 14, which comes early after only 380 ms, has aberrancy.
The prehospital strip with a run of 6 beats had the same RBBB morphology. Therefore that was NOT a run of VT, but several aberrant beats in succession.
In that rhythm strip, the beat preceding those beats did occur after a long preceding R-R interval, but the others did not. If all the succeeding beats come very early, (“long-short” without the long), then there can be aberrancy without the preceding long R-R interval.