A 50 something presented with 10/10 bilateral arm and pain between the shoulder blades that started at work. It felt like a “tearing,” and was associated with diaphoresis.
BP was 250/140. He appeared distressed.
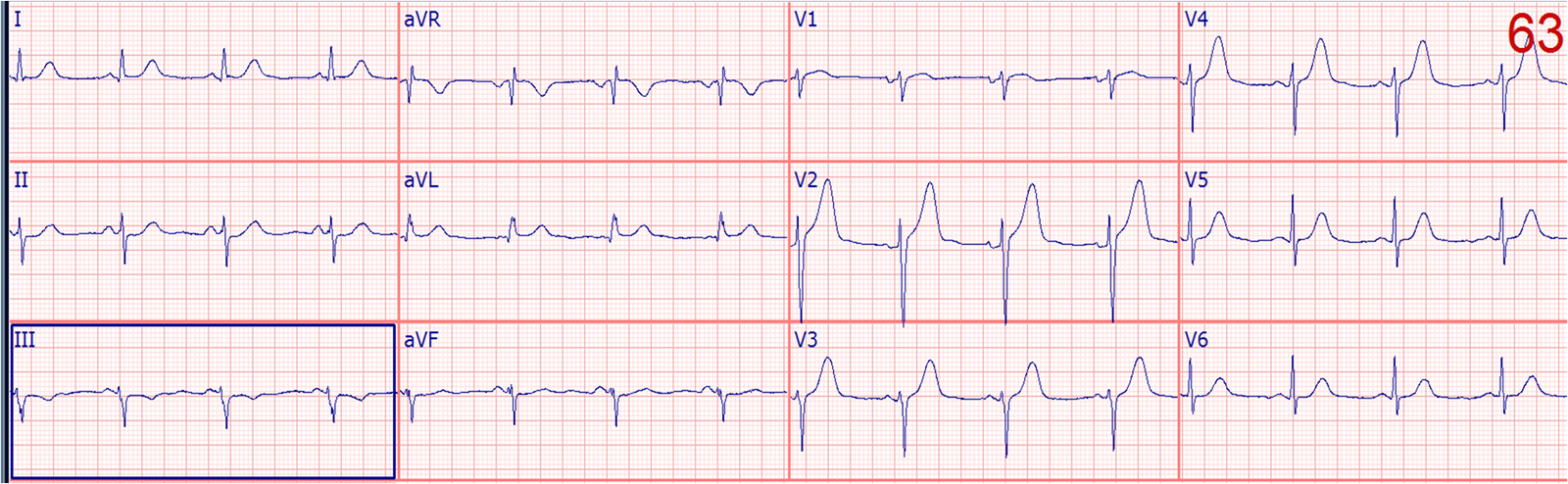
Here is the initial ECG:
 |
| This is diagnostic of inferoposterior MI, with acute coronary occlusion.
There are hyperacute T-waves in inferior leads, ST depression and T-wave inversion in aVL, and ST depression with T-wave inversion in V2 and V3. There is also ST depression in V4-V6. |
Of course the initial fear was aortic dissection, with the classic pain and severely elevated BP. And it is not uncommon for a dissection to dissect down the coronary arteries, especially the RCA, so one might find an ECG like this in aortic dissection. (Though only a tiny minority of RCA STEMI are caused by aortic dissection!)
The patient was given labetolol without much effect, then esmolol and nitroprusside until the BP was under control.
He was sent to the CT scanner where no dissection was found.
At this point the ECG findings must be attributed to acute coronary syndrome. A repeat ECG is indicated to look for evolution or resolution.
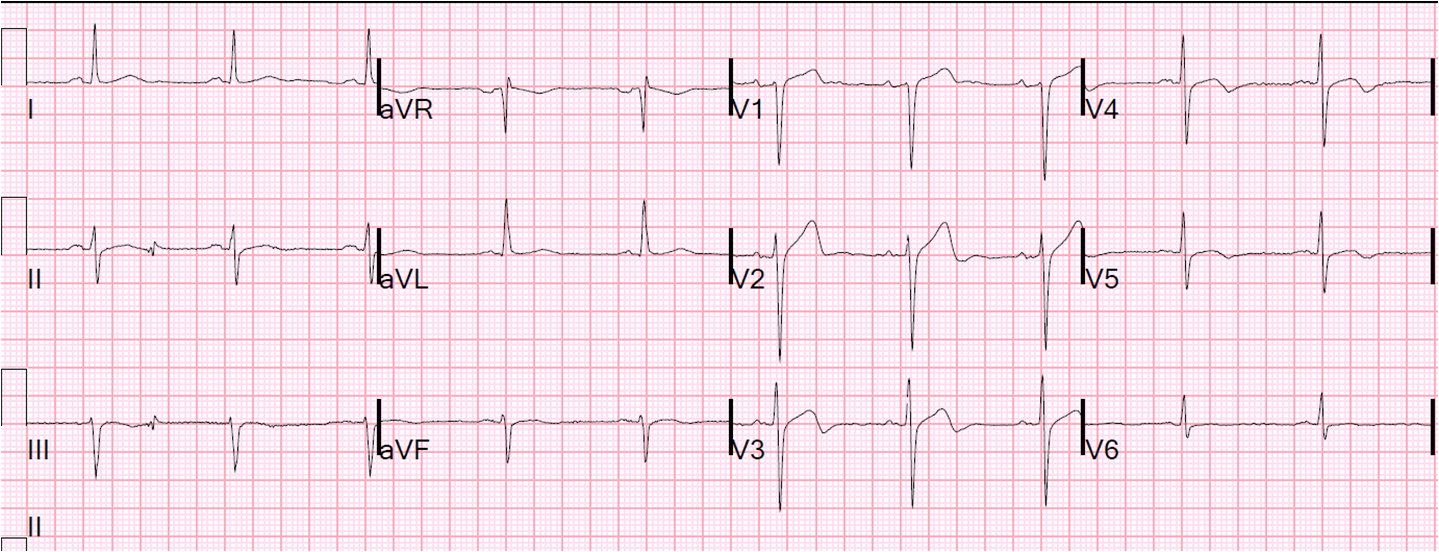
Before another ECG was obtained, the pain resolved. This was recorded at 90 minutes:
 |
| Normalization was attributed to normalization of the severely elevated BP. |
The first troponin was slightly elevated. The ischemia was thought to be due to severe hypertension (a type 2 MI). The cath lab was not activated.
Only less than 5% of type 2 MI present with subepicardial ischemia (ST elevation). Demand ischemia from hypertension would be unlikely to manifest such focal STEMI on the ECG.
Progress
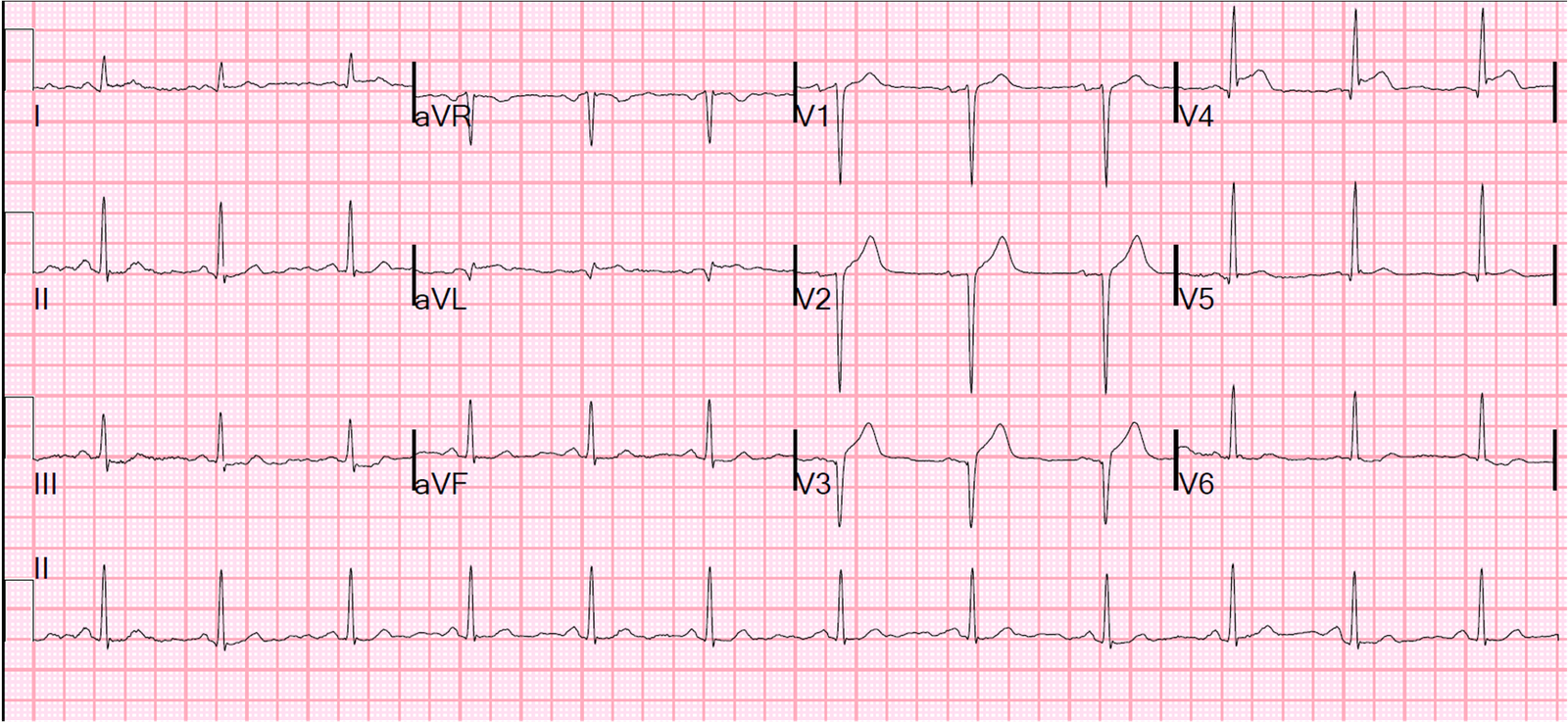
While waiting for a bed, he developed chest pain again, and this ECG was recorded at 120 minutes:
 |
| Now there is obvious inferoposterior STEMI |
The cath lab was activated.
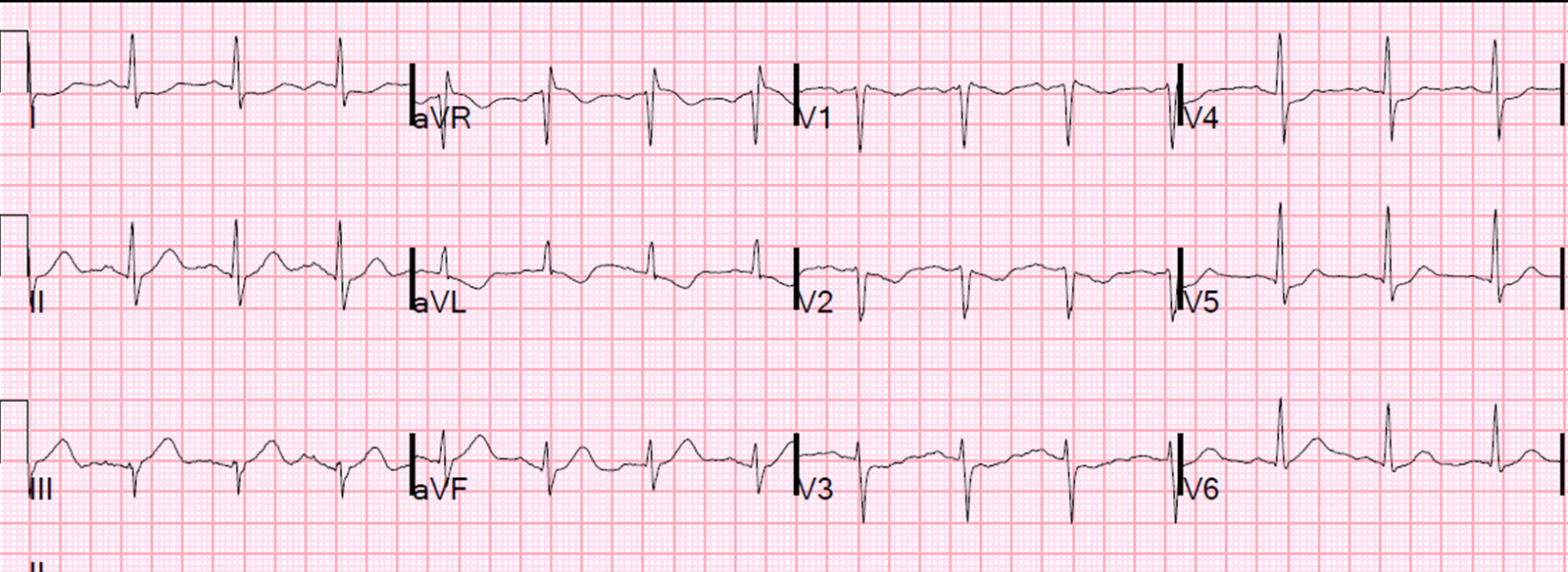
While waiting, the pain subsided again 10 minutes later (recorded at 130 minutes):
 |
| ST segments and hyperacute T-waves have normalized. |
10 minutes later, the pain recurred again (time 140 minutes):
 |
| Obvious STEMI again. |
Cath showed a 100% thrombotic occlusion of the RPAV off the RCA, stented.
Reperfusion was so fast that there was no wall motion abnormality the next day.