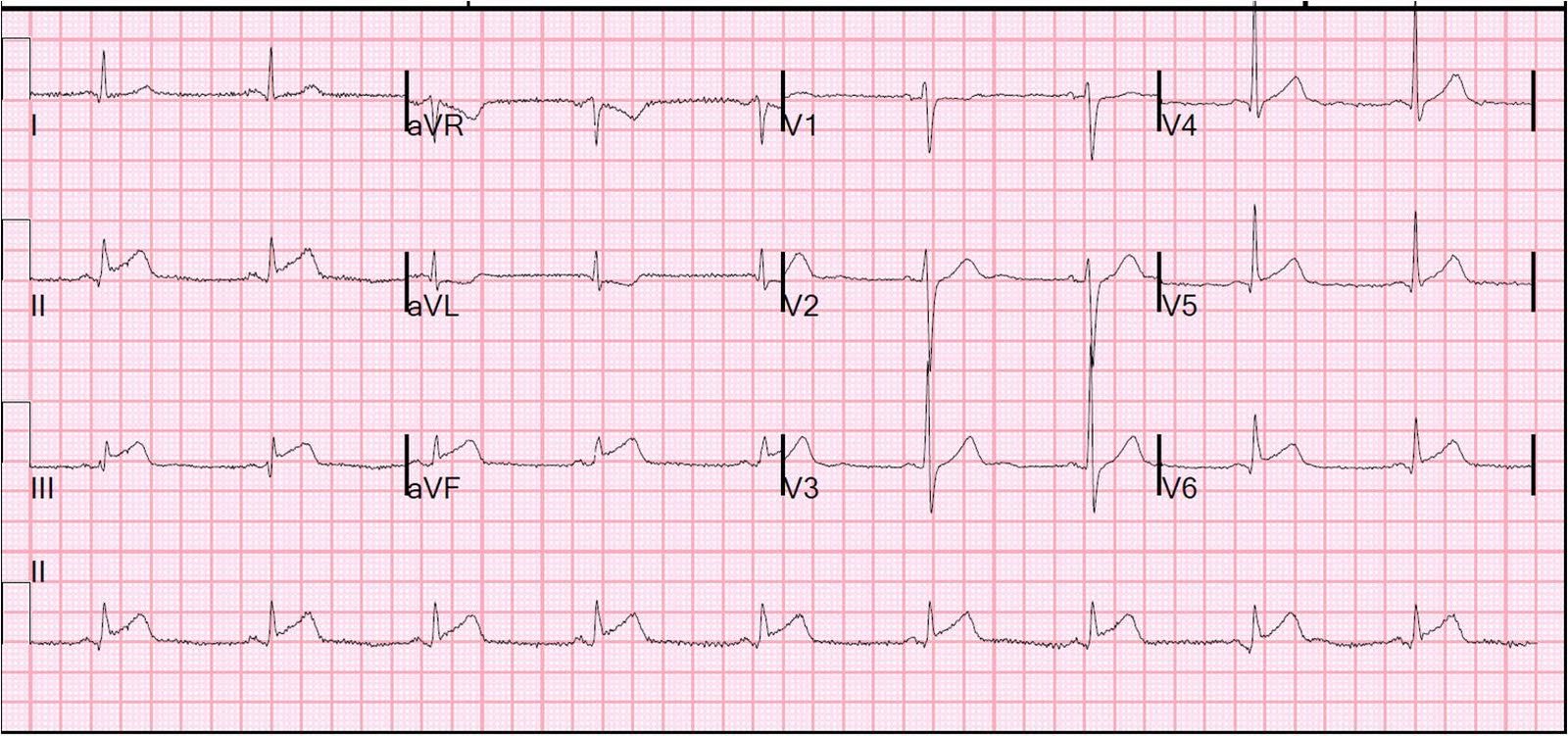
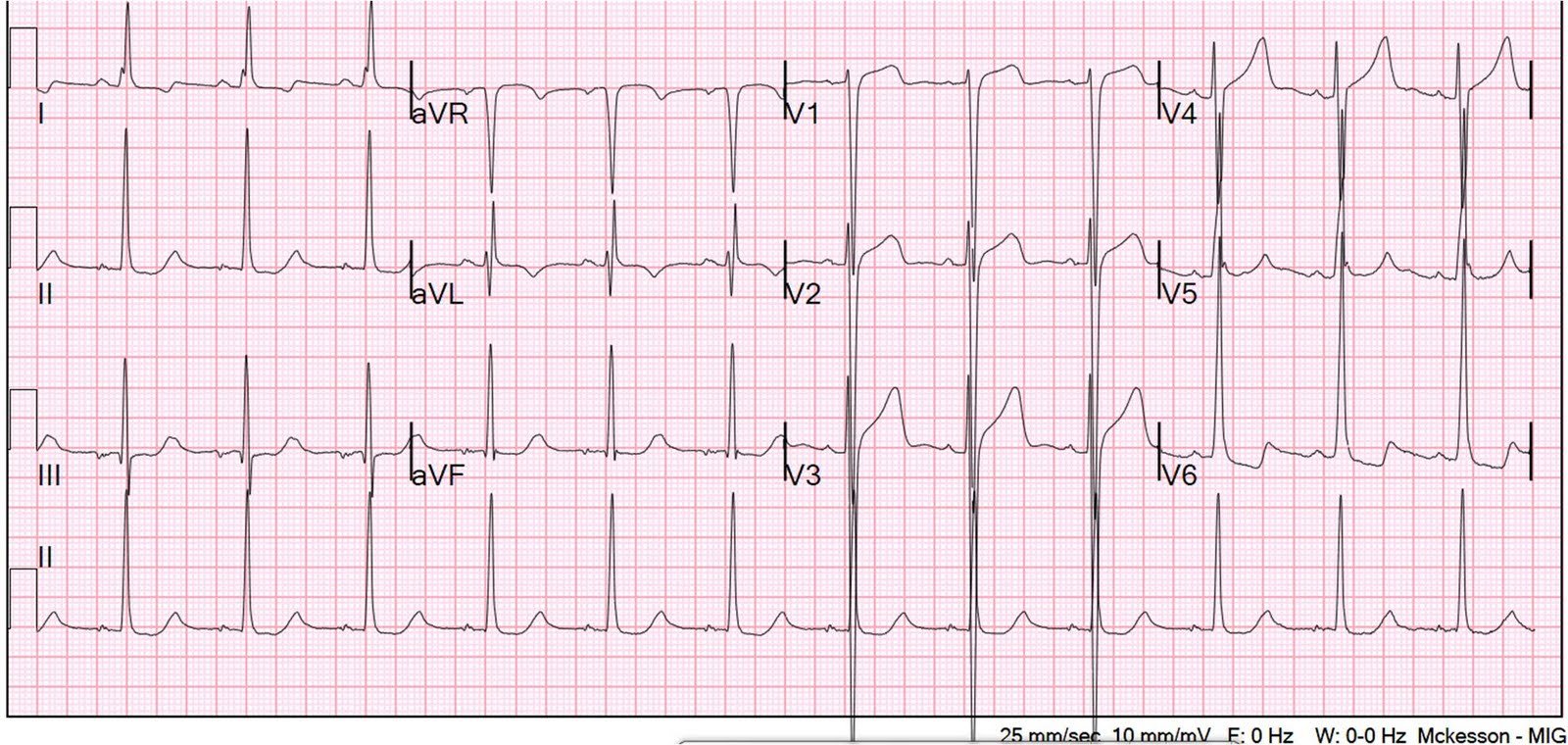
This young male had ventricular fibrillation during a triathlon. He was resuscitated with chest compressions and defibrillation and 1 mg of epinephrine. On his bib it stated that he had a congenital heart disorder. He arrived in the emergency department hemodynamically stable. His initial ECG is shown here.
There is profound LVH with anterolateral ST elevation and reciprocal ST depression in II, III, aVF, and ST depression in V5 and V6 that could all be secondary to LVH or could represent ischemia superimposed on the repolarization abnormalities of LVH: note that wherever there is ST depression, it is associated with a very high voltage R-wave. The ST elevation in V1-V3 is typical of LVH (high voltage S-waves), but the ST elevation in aVL is concordant to (in the same direction as) the high voltage and thus very suggestive of injury pattern.
ACS would be highly unusual in a young athlete, and given the information on his race bib, one must first suspect that the abnormal ST elevation is due to demand ischemia, not ACS.
A bedside echo performed by the emergency physician showed no wall
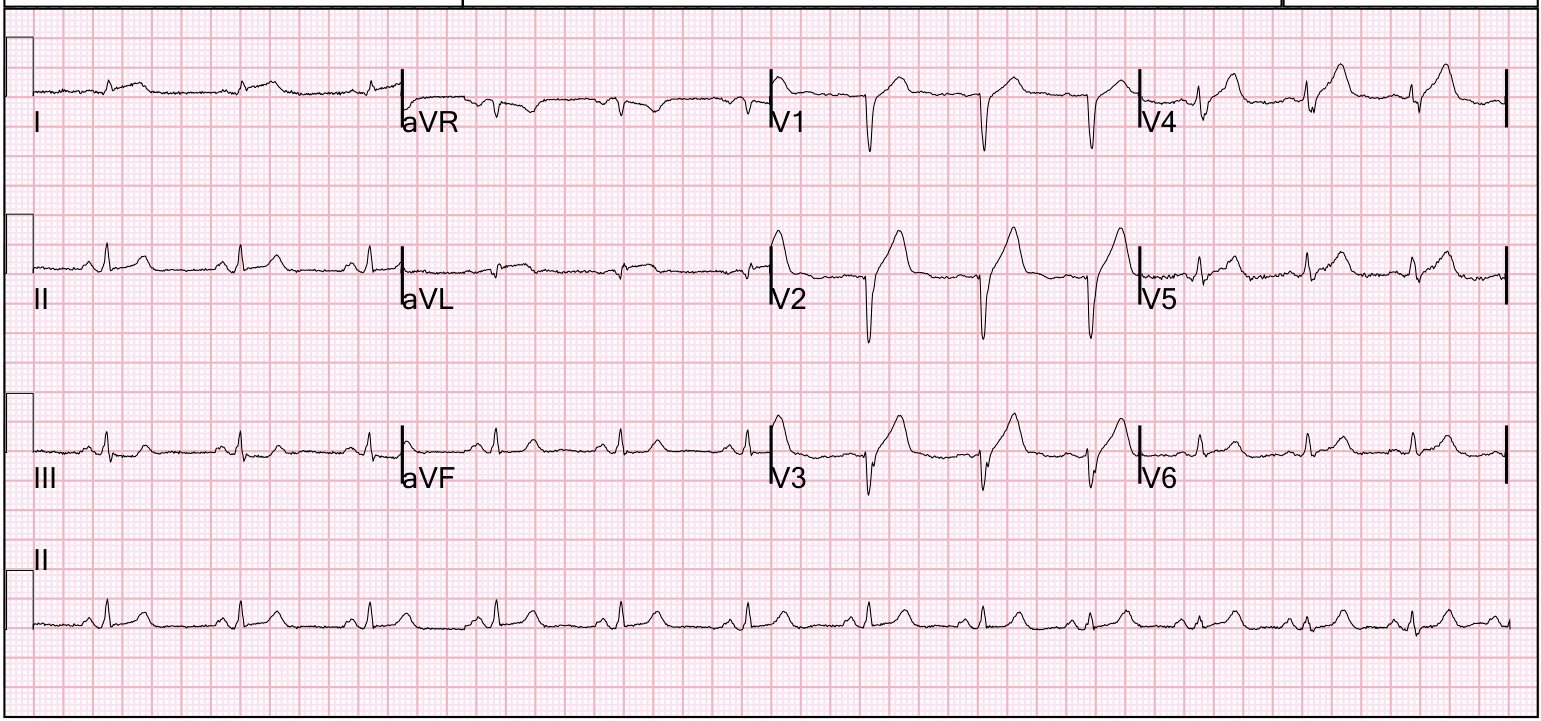
motion abnormality and confirmed LVH. A repeat ECG after a few minutes of cool down is shown.
| Now there is much less ST segment deviation, less elevation and less depression. |
The troponin returned positive, and the maximum troponin was 3.8 ng/ml. The next day, and angiogram showed normal coronary arteries. An echocardiogram confirmed aortic stenosis with a large pressure gradient. The stress of the triathlon cause demand ischemia and ventricular fibrillation. He awoke and did well.
Thus, this patient had increased ST elevation (current of injury) superimposed on the ST elevation of LVH and simulating STEMI.