A middle aged male with history of bicuspid aortic valve and aortic stenosis complained of 30 minutes of chest pain and dyspnea. He described it as tightness and pressure. Vital signs were normal and he appeared well.
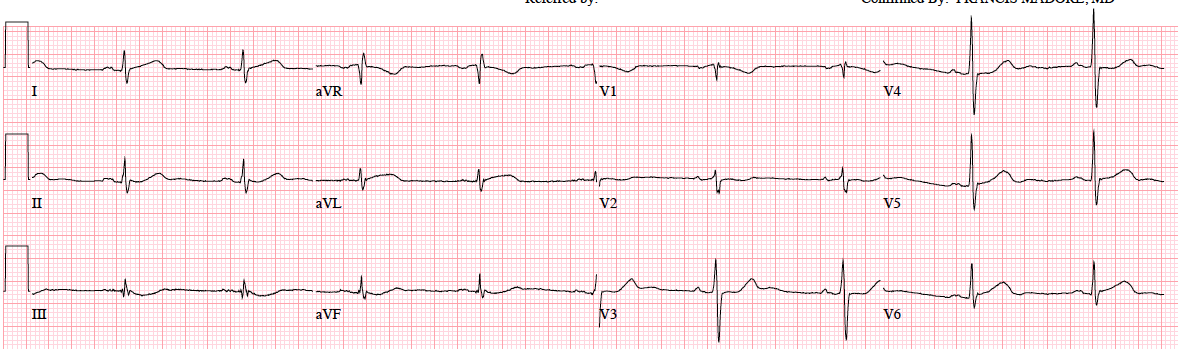
Here is the initial ECG:
 |
| There is profound LVH with incomplete LBBB, with a QRS of 118 ms. There is marked ST elevation in precordial leads. Although this can be seen with this degree of LVH and incomplete LBBB, one must entertain the possibility of anterior STEMI. The ST/S ratio is 5/28 in lead V2, for a ratio of 0.18. Though 0.18 is less than 0.25, and of course also less than 0.20, it is still quite a high ratio. A mean maximal ST/S ratio for a cohort of patients with complete LBBB is 0.10 (95% CI: 0.9-0.11). |
Worried about STEMI, a bedside echo was immediately recorded. Here is the parasternal long axis:
There is profound LVH and good wall motion
Here is a still image:
 |
| The arrows highlight the wide aortic root |
A parasternal short axis was done:
This shows profound LVH with overall good wall motion. In particular, the anterior wall and septum have good wall motion. This makes anterior STEMI very unlikely.
The aortic root was not initially noticed, but the physicians were confident there was no STEMI.
Suddenly the pain resolved spontaneously after 45 minutes.
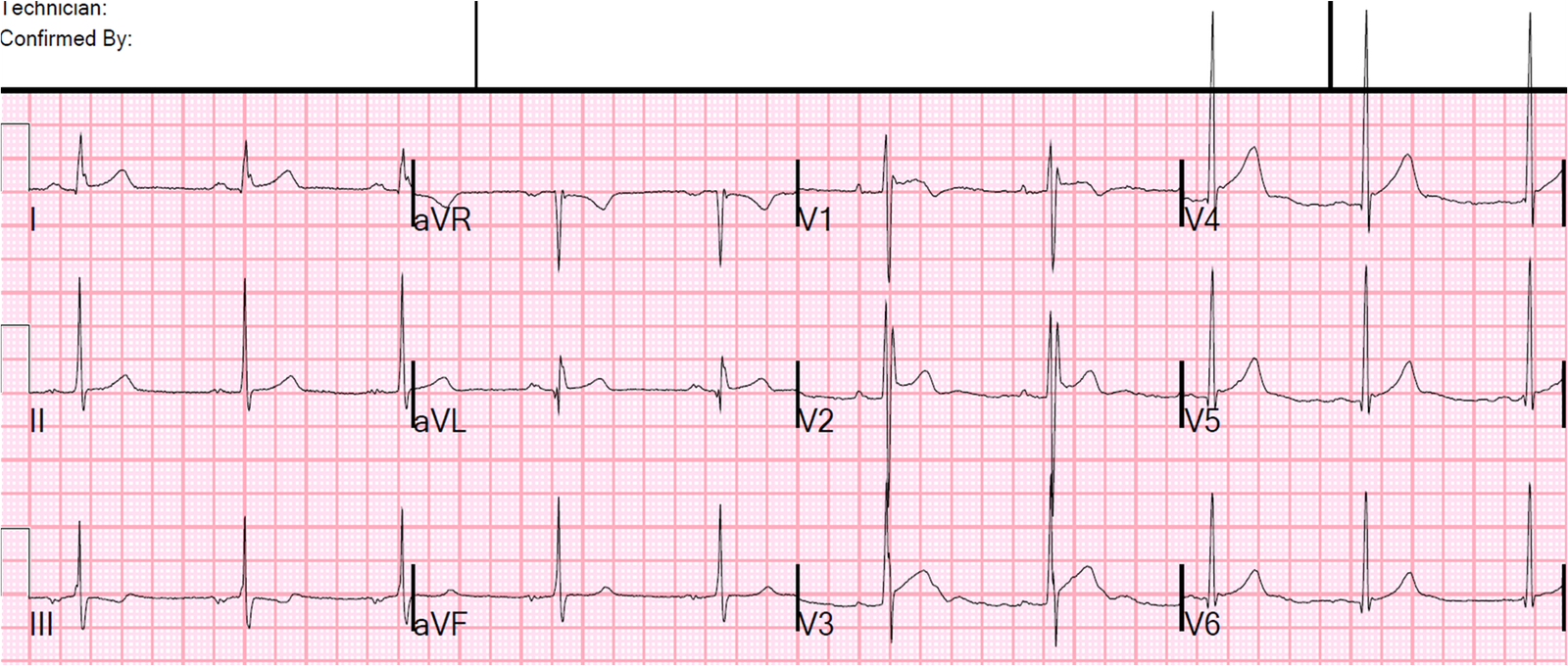
The initial troponin I returned elevated at 0.128 ng/mL, at which point another ECG was recorded:
 |
| No change, consistent with the interpretation that this is the baseline ECG |
The on-call cardiologist was consulted for management of this patient with a positive troponin and worrisome ST segments. Because of the history of bicuspid aortic valve, the cardiologist was concerned about possible Aortic Dissection and suggested a chest CT.
After a second look at the echo, there was more suspicion of dissection, and a CT was ordered. Here is one image:
 |
| This shows a large aortic root aneurysm that also has a subtle dissection (low density thin lines in the midst of the contrast is a dissection flap) |
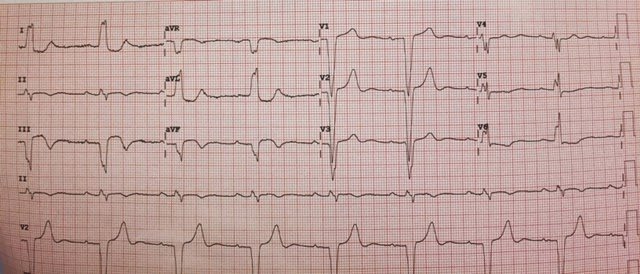
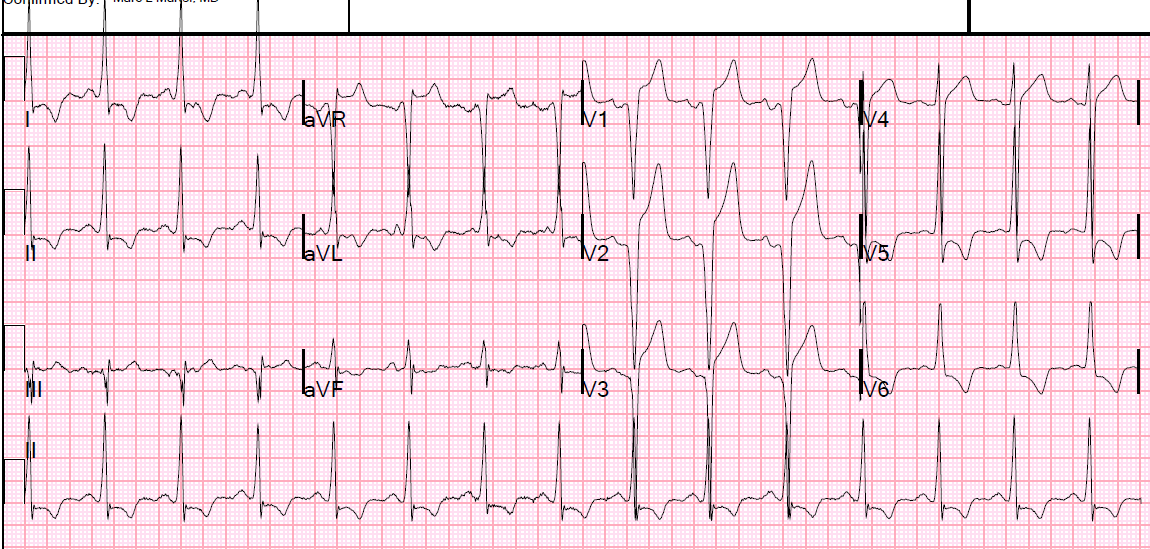
A repeat ECG was essentially unchanged.
 |
| Consistent with massive LVH |
The patient went to the Operating Room.
(I am not completely certain that there was no involvement of the coronary cusps, with resulting partial occlusion of the left main and resulting NonSTEMI, but the serial ECGs do not support this).
A later transesophageal echo showed that the initial dissection flap obstructed the right coronary cusp and resulted in occlusion of the RCA, but then a hole in the flap developed which restored flow to the RCA. This is probably why the pain was relieved after 45 minutes.
Learning points:
1) Massive LVH can evolve over time to incomplete, or complete, LBBB, and it can have ST elevation that mimics STEMI.
2) Use ED echo to confirm good wall motion when there is anterior ST elevation due to LVH
3) Don’t forget aortic dissection!