A Middle-aged male had sudden onset severe substernal chest pain that woke him from sleep.
His BP was 238/118 on arrival.
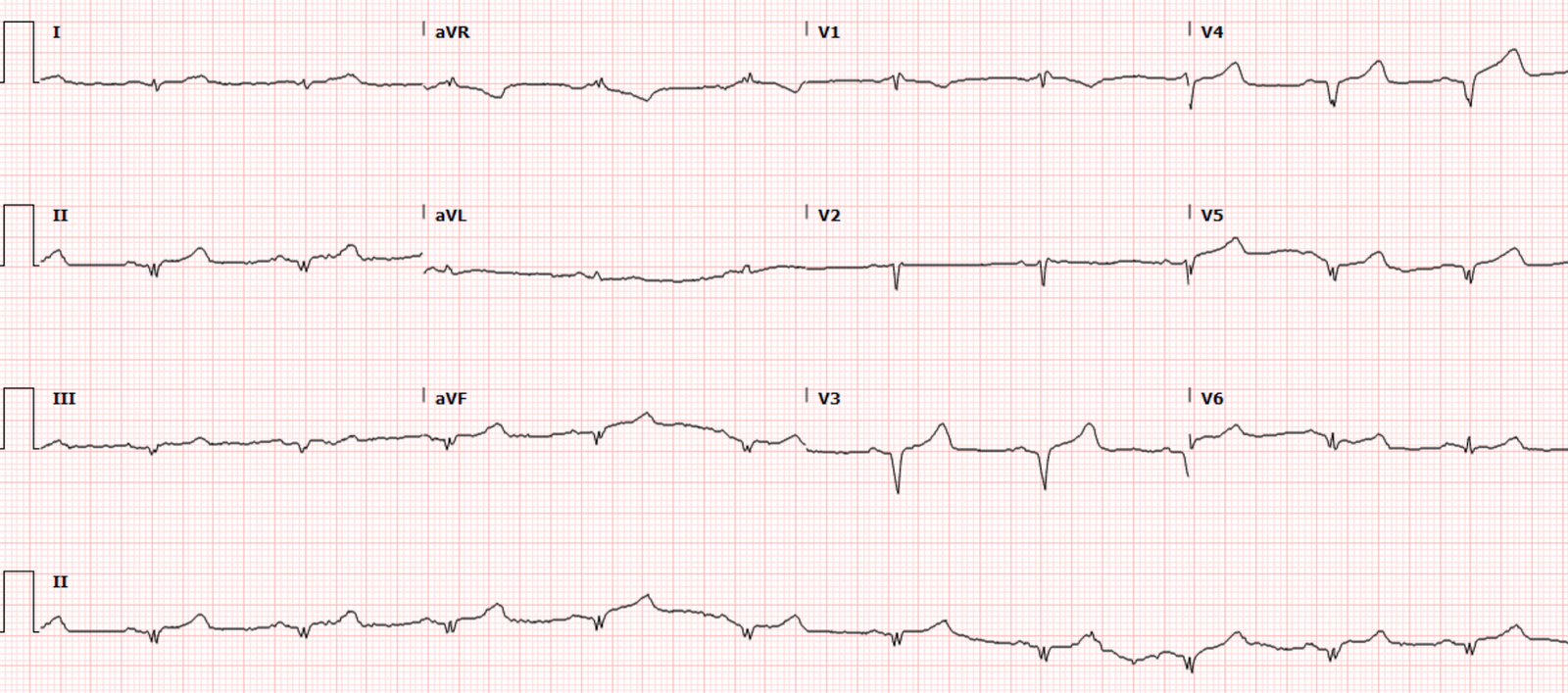
Here is his first ED ECG:
What do you think?
There is ST depression maximal in V2-V4, which normally would be all but diagnostic for posterior MI. However, the extremely elevated BP makes it likely that this STD is really subendocardial ischemia from high oxygen demand. (There are also incidentally large U-waves — the K was 4.1).
It is best to first manage the BP and then repeat the ECG.
So the physician did just that. He obtained a chest CT to rule out aortic dissection (which was negative).
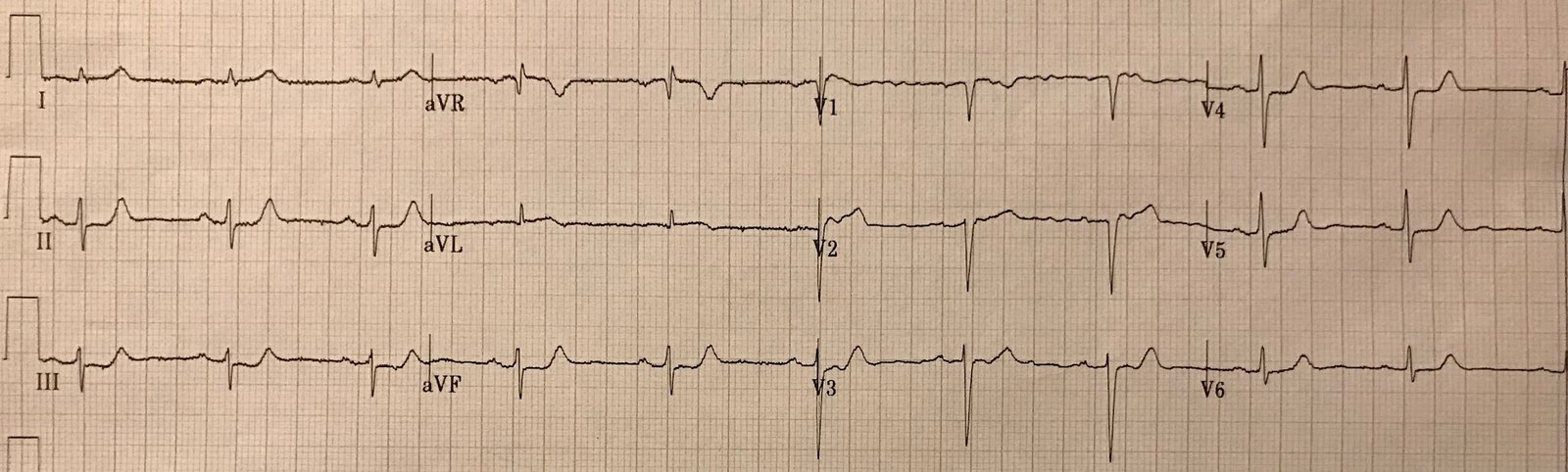
He also gave nitroglycerine to bring the Systolic BP down to 180 mmHg, at which time the chest pain resolved. Then he recorded another ECG:

The ST depression and pain is gone! It must have been demand ischemia, right?
He gave aspirin, heparin and transferred to the nearest PCI center.
The initial troponin at that referral center was “negative”, so they observed the patient. A later troponin returned at 0.346 ng/mL (unfortunately, I don’t have the assay — don’t even know if TnI or TnT. In any case, that level is elevated and diagnostic of either type 1 or type 2 MI).
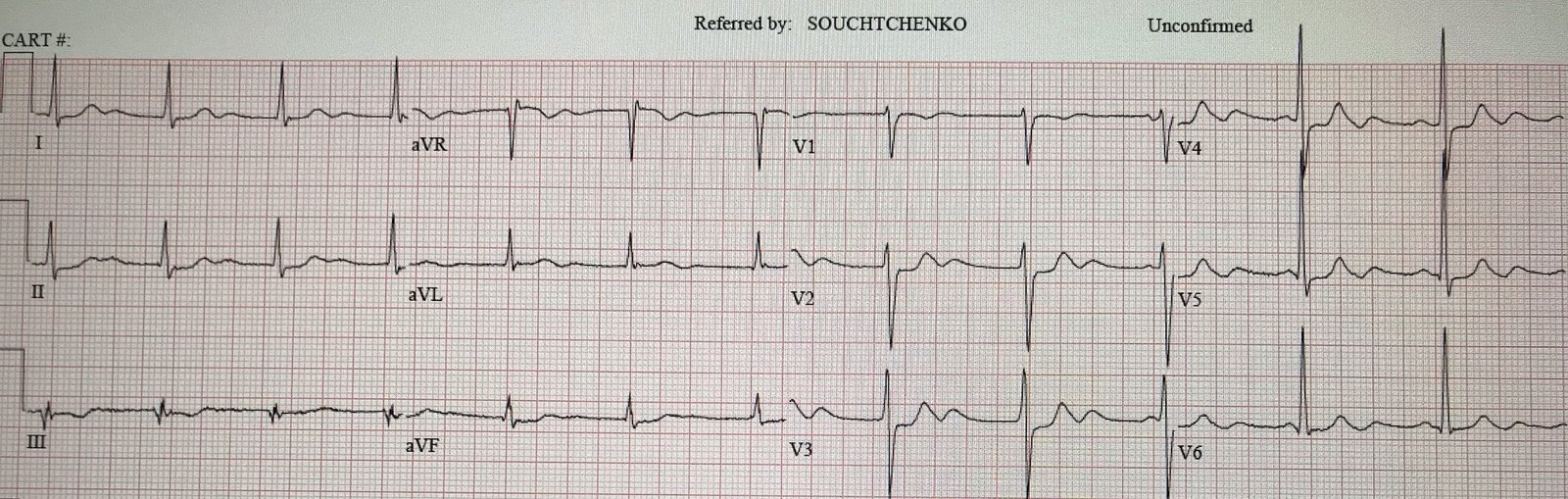
Shortly thereafter, the patient had sudden onset 10/10 pain again. Another ECG was recorded:

The ST depression is back!
He went for emergent angiogram and was found to have a 100% proximal circumflex occlusion with TIMI-0 flow.
Comment:
The physician was worried that he had made a mistake here.
I disagreed.
One must manage very abnormal vital signs first. There is no way to know whether the initial chest pain + EKG findings were not subendocardial ischemia due to high oxygen demand due to the extremely elevated BP.
The correct management is to manage the BP, then assess symptoms and a repeat ECG.
As it turned out, the ischemia was indeed due to ACS.
It is an unfortunate coincidence that the artery spontaneously opened (reperfused) at the same time that the BP was managed. The physician could not have known that.
It was only when the ischemia returned (both symptoms AND ECG findings, in this case) WITHOUT an elevated blood pressure that it could be ascertained that this was all due to coronary occlusion.
The ECG did indeed look more like posterior OMI than subendocardial ischemia
One certainly might strongly suspect that this is ischemia is due to posterior OMI rather than subendocardial ischemia, since posterior OMI usually has maximal STD in V2-V4, and subendocardial ischemia usually has STD in I, II, V4-V6, with reciprocal STE in aVR
See here for a case of LAD subendocardial ischemia that presented like a posterior OMI; it even had STE on posterior leads. Guess the culprit with ST Elevation in posterior leads
Summary: The physician was thrown a curveball, but he managed it very well. (That is a baseball metaphor, for those outside the U.S.!)
A particularly difficult issue, obstacle, or problem. Named after the equally tricky baseball pitch.
The professor really threw me a curve ball with that last exam test.