Or at least understand their limitations!!
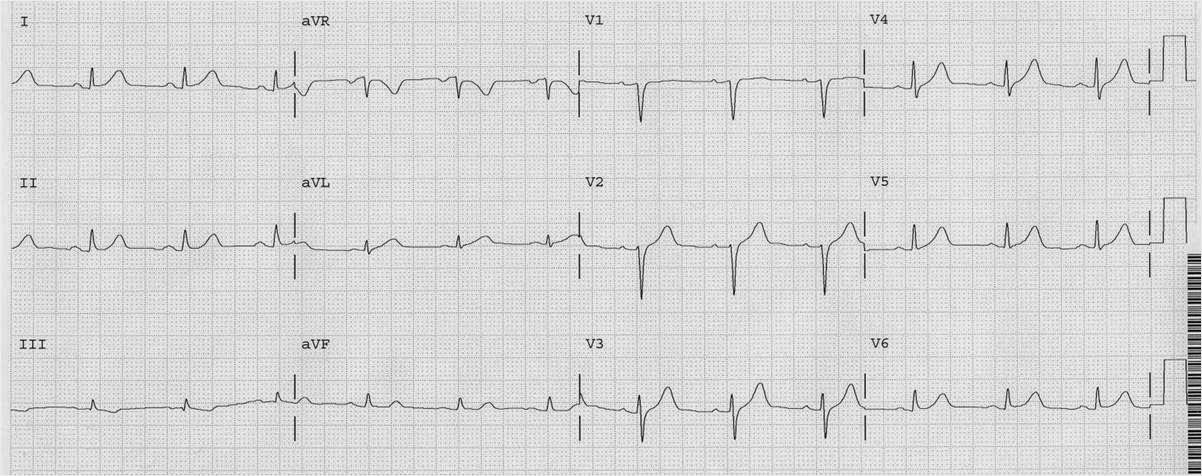
This patient had chest pain and this ECG:
 |
| There is no significant ST elevation. But there is ischemic ST depression in V2-V6. It is maximal in V3 and V4, which represents posterior STEMI until proven otherwise. |
(This can be due to subendocardial ischemia, but less likely. Most subendocardial ischemia is diffuse, with the ST depression vector pointing towards the apex of the heart (II, V5) and thus has maximal ST depression out in V5 and V6.
The ST elevation vector is clearly away from V3 and V4, towards the posterior wall. If you put posterior leads on, you MUST get posterior ST elevation. HOWEVER, it may be of very small magnitude and thus is may be a false negative.
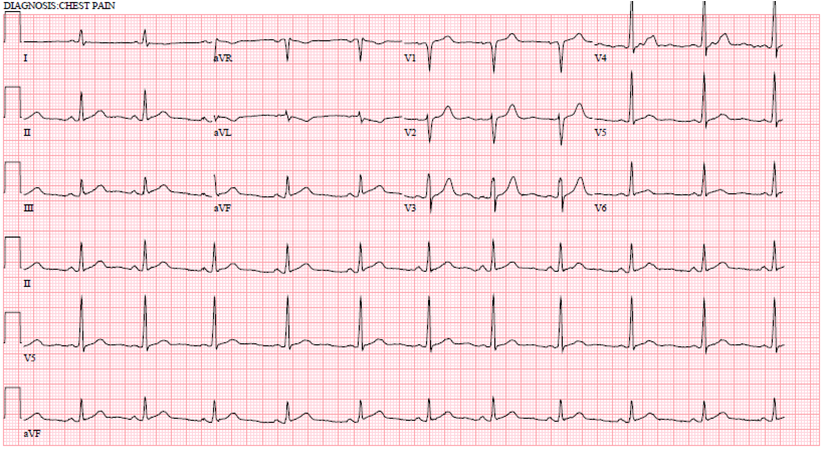
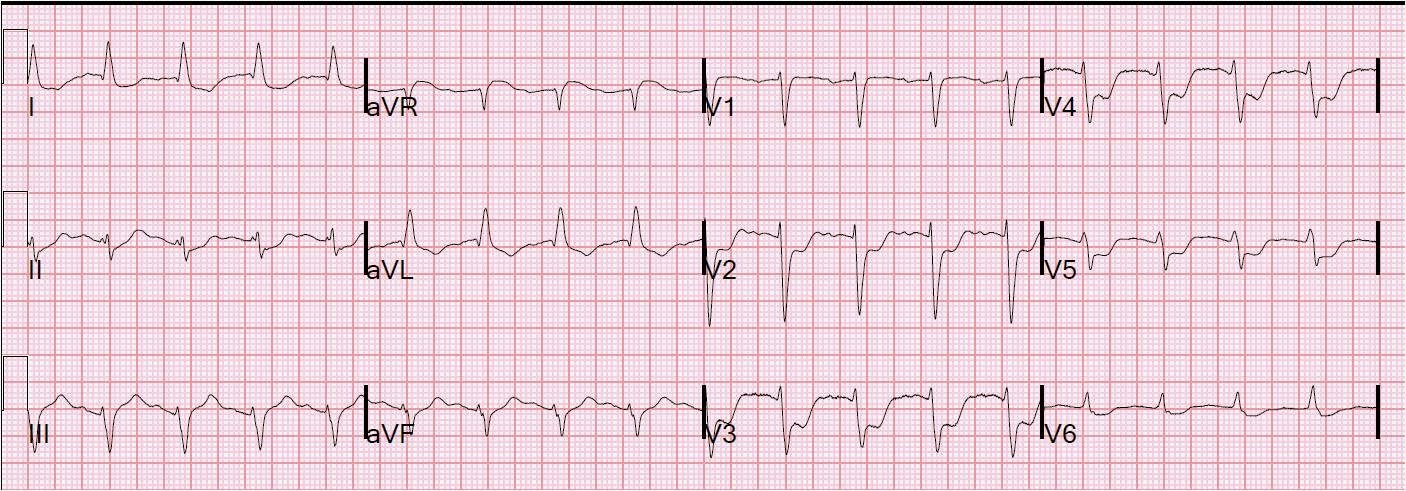
Posterior leads were applied:
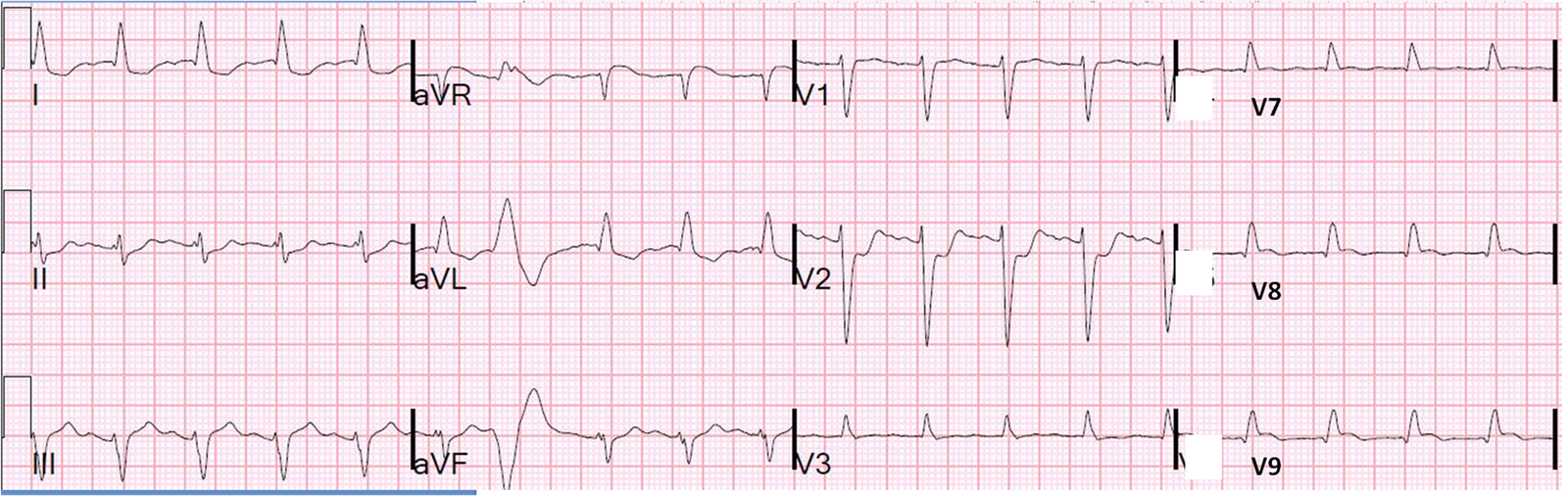 |
| V3 is misplaced here, so ignore it. Notice there is some ST elevation in V7-V9, but it is minimal. It does not even meet the “criteria” of 0.5 mm in posterior leads. V2 has the same ST depression in had on the first ECG, confirming that the artery is still closed. |
So this gives a false negative. Posterior leads lead you astray. The voltage is so small that you might be dissuaded from your diagnosis of posterior MI.
This was indeed a circumflex occlusion with a posterior wall motion abnormality.
So when should you use posterior leads?
There is some literature showing that some posterior MI show up only on anterior precordial leads as ST depression, and some show only on posterior leads.
I think some of this is due to timing. Arteries open and close and if you don’t record the ECGs simultaneous, then you might be recording two different conditions of ischemia.
It may be useful to record posterior leads in a patient in whom you are convinced has an MI but has no significant abnormalities on the standard 12-lead.