Case 1.
A younger middle-aged male called EMS for chest pain. They recorded a prehospital ECG which I do not have, but they did a prehospital cath lab activation for chest pain and inferolateral ST elevation.
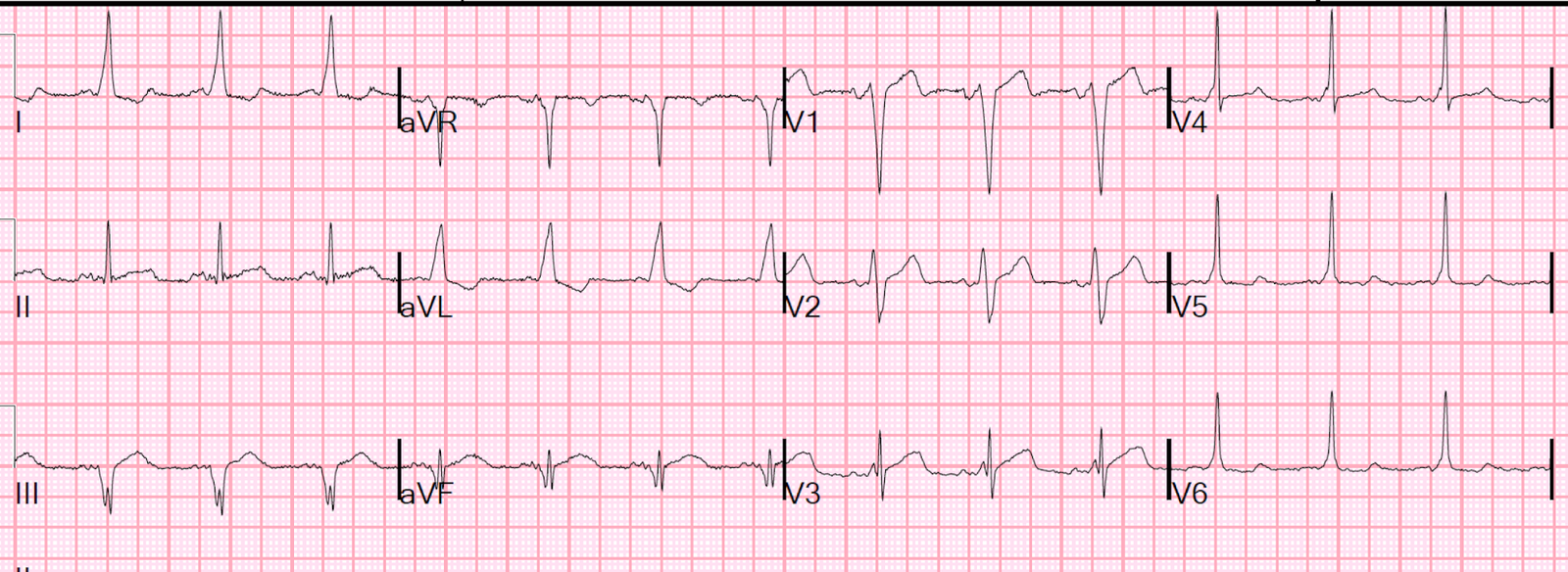
Here is the ED ECG:
 |
|
There is inferior ST elevation and also ST elevation in V5 and V6. Is this inferior and lateral STEMI? |
Case 2.
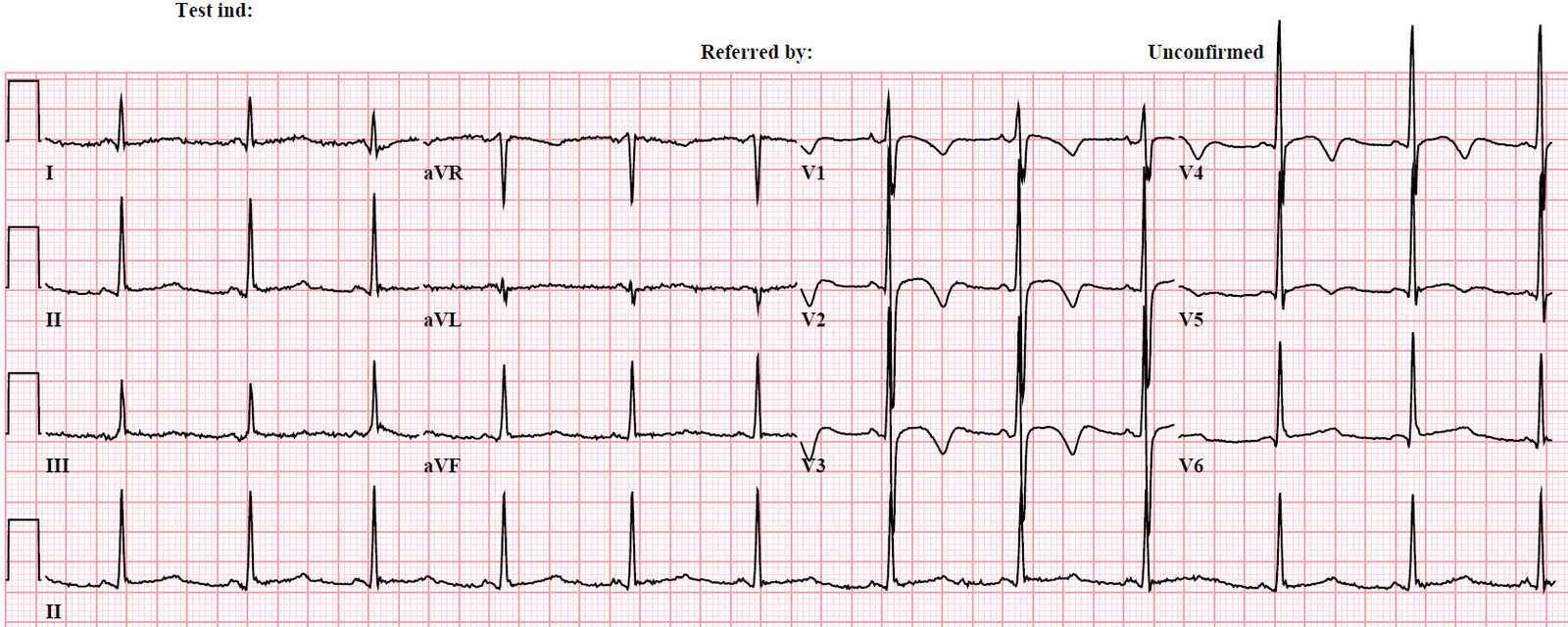
A middle-aged male presented with chest pain:
 |
| There is inferior ST elevation and also ST elevation in V5 and V6.
Is this inferior and lateral STEMI? |
Case 1 is typical early repolarization. A stat echo was negative, the cath lab was cancelled, and serial ECGs were negative. Other aspects which strongly suggest early repol are: 1) high voltage in leads with ST elevation; 2) proportionally small T-waves and ST elevation in these leads.
Case 2 is typical pericarditis (and was, indeed, proven pericarditis). The absence of reciprocal ST depression in lead aVL makes it very unlikely to be inferior MI, even when there is ST elevation in V5 and V6.
Learning point: The absence of reciprocal ST depression in lead aVL makes it very unlikely to be inferior MI, even when there is ST elevation in V5 and V6.
But wouldn’t there always be ST elevation in aVL if there is STE in V5 and V6?
No!
V5 and V6 are lower down and more like lead II than like aVL.
Case 3.
This patient presented with one hour of chest pain.
 |
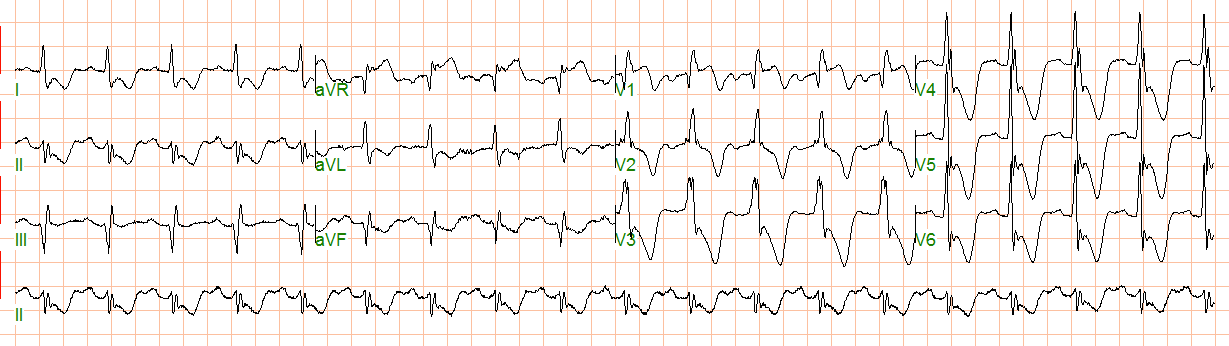
| The diagnosis of inferior-posterior-lateral STEMI is obvious, but look at the huge ST elevation in V5 and V6. Nevertheless, there is a small amount of reciprocal ST depression in lead aVL. |
With such high ST elevation in V5 and V6, wouldn’t you expect an absence of ST depression in lateral lead aVL, or even ST elevation in aVL?
No!
We found in our study of inferior MI (http://www.ajemjournal.com/article/S0735-6757(15)00818-9/abstract) that: of patients whose ECGs had inferior ST elevation due to STEMI and also had ST elevation in V5 and V6, 35 out of 35 (100%!) had some ST depression in lead aVL.
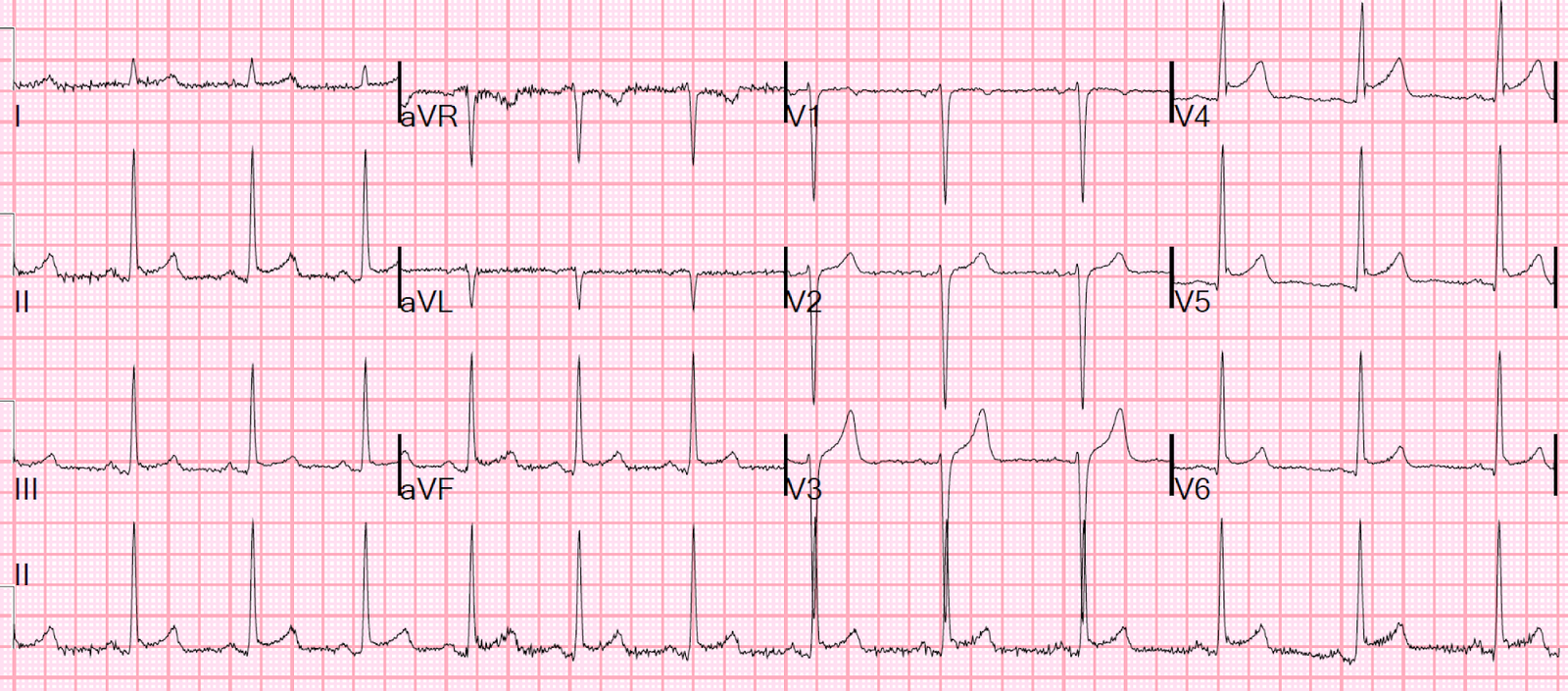
This is helpful in cases such as these:
 |
| There is inferior ST elevation and also ST elevation in V5 and V6. However, there is no reciprocal ST depression in aVL. This was early repolarization. |
 |
|
|
Learning Point:
If there is inferior ST elevation, but no reciprocal ST depression in aVL, you should be skeptical of the diagnosis of STEMI even if there is ST elevation in V5 and V6.