Dr. Josu Abecia Valencia, from Spain, asked me my opinion on this case. He has a great Spanish language blog. You can find this case in Spanish at his blog here: https://urgenciasbidasoa.wordpress.com/2015/11/16/caso-201-varon-de-35-anos-con-dolor-toracico-de-10-horas-de-evolucion/
He gave his permission for me to post it here.
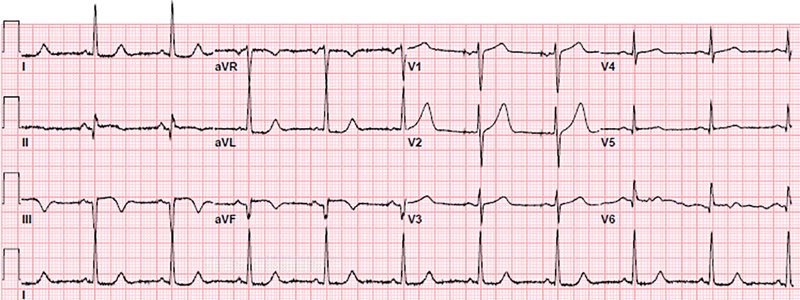
A 35 year old complained of typical substernal chest pain:
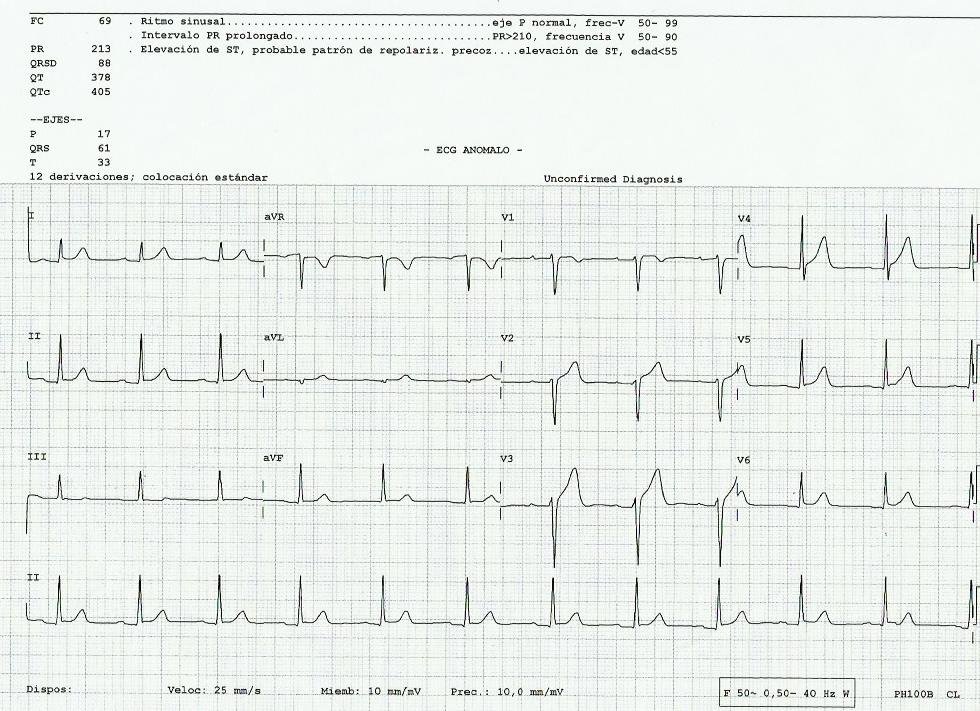 |
| What do you think? My opinion is below. Notice the computer reads early repolarization. |
Here is my response:
Dr. Abecia,
This is highly suspicious for LAD occlusion, though not diagnostic.
Have you used my formula?
ST elevation at 60 ms after the J point in lead V3 = 4 mm
computerized QTc = 405
R-wave amplitude in V4 = 14.5 mm
Formula value = 23.9, which is > 23.4 which is pretty specific for LAD occlusion.
I would do frequent serial EKGs, every 15 minutes, for several hours.
I would do an emergent formal contrast echocardiogram.
If still non diagnostic, consider immediate angiography.
What was the outcome?
Here is the outcome (slightly limited because I don’t read Spanish very well):
Time zero: Troponin T drawn, returns later at 43 ng/L (= 0.043 ng/mL, slightly elevated)
Serial EKGs unchanged.
Thoughts: myopericarditis vs. early repolarization vs. possible MI
Time 5 hours: Troponin T returns at 151 ng/mL.
Still thinking myocarditis
Time 11 hours: Troponin T returns at 350 ng/mL
Echo shows EF of 67% and no Wall Motion Abnormality
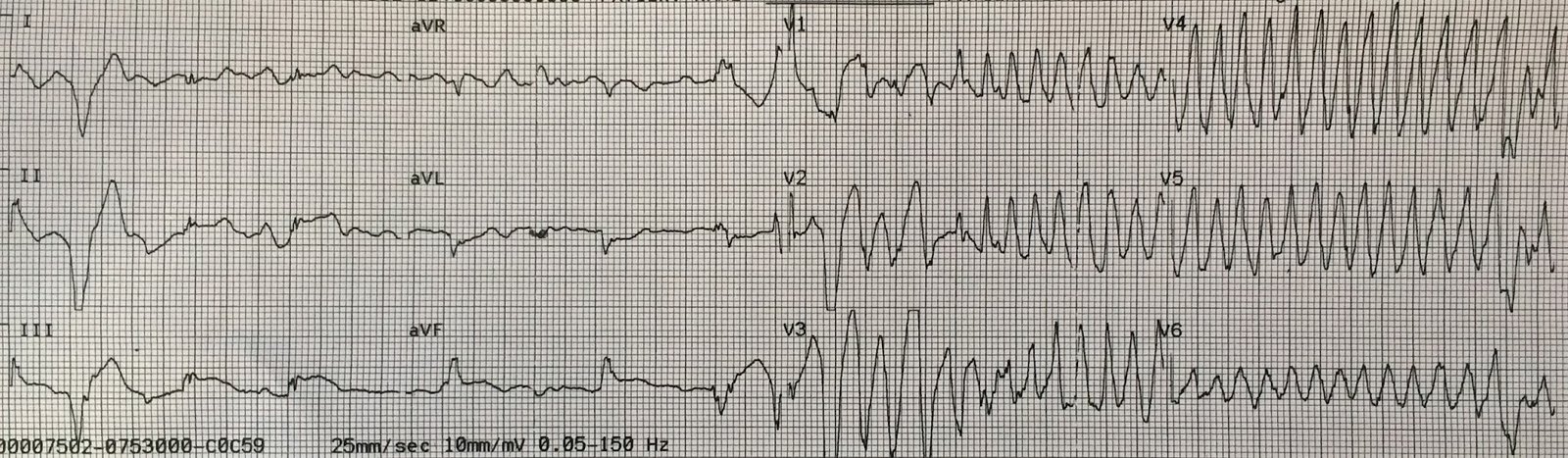
But symptoms persisted, and with the positive troponin, they sent him for angiogram. Here are the results:
 |
| Occlusion of the very distal LAD. So in this case, it was a small infarct territory. The thrombus was suctioned out and it was stented. Symptoms resolved. |
The formula to differentiate benign ST elevation from LAD occlusion worked perfectly, even though it was a small anterior MI. It outperformed serial ECGs and formal echocardiogram.
One might argue, with good rationale, that such a small MI can wait until the next day for angiogram. I will not oppose the argument strongly, but the patient did have ongoing chest pain that was relieved by intervention.