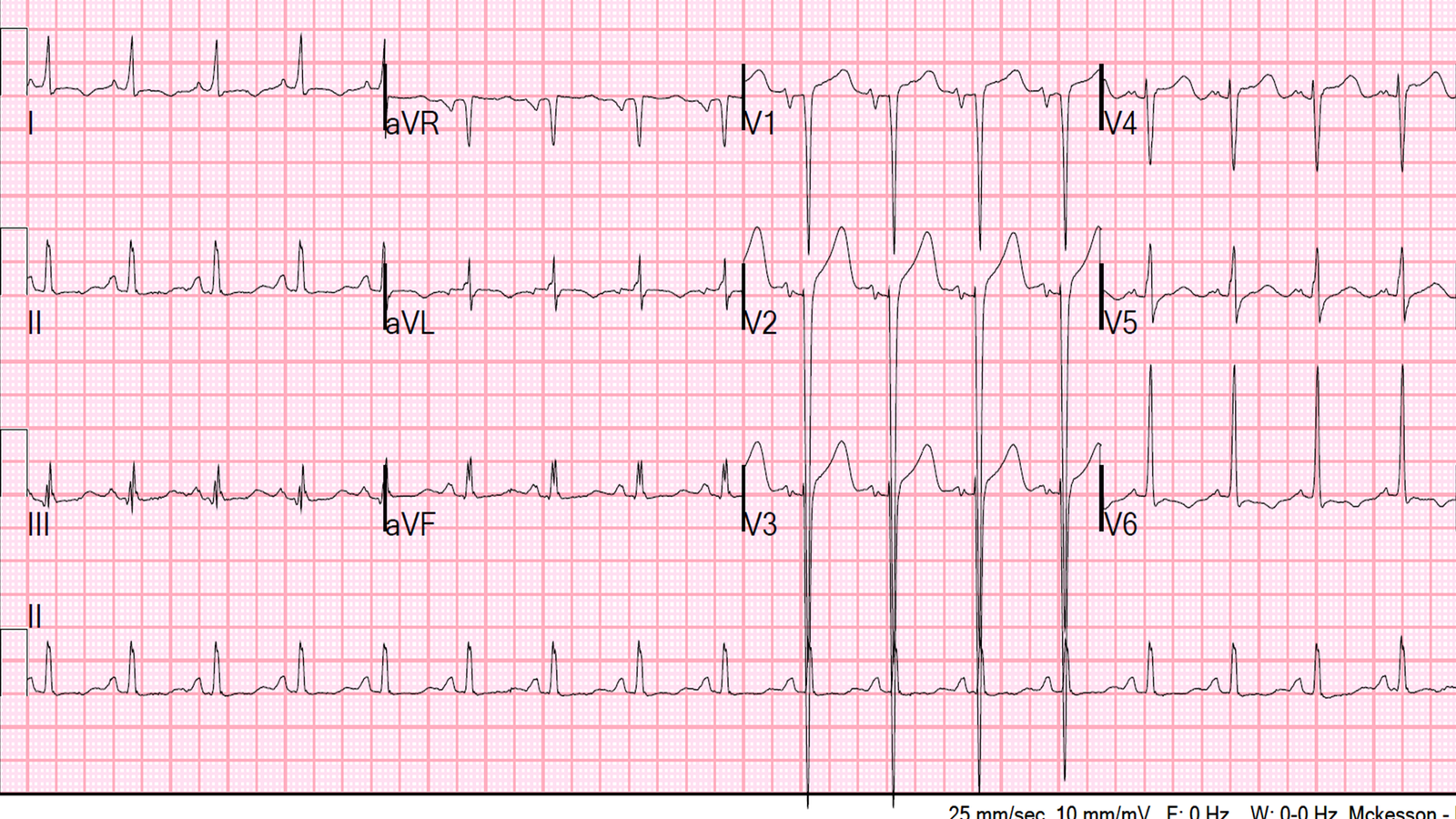
A woman in her 30’s with h/o HTN presented with atypical chest pain after a stressful event. Here is her ED ECG:
 |
| There is sinus tachycardia. There are very large anterior T-waves, with ST elevation. However, there is also very high voltage. Criteria for LVH is clearly reached in aVL, with tyical repolarization (“strain”) in aVL. The ST elevation and tall T-waves are discordant to deep S-waves in V2 and V3. |
I took care of this patient and was concerned about the ST-T waves in V2 and V3, but thought that they were almost certainly a result of LVH. One should not apply the LAD occlusion vs. Benign Early Repol Formula if the patient has LVH. Had I done so, with a QTc of 375ms, the formula value would have been 26.1, indicating anterior STEMI. Here is another example of LVH resulting in a falsely positive formula value.
I think that the formula would be more accurate if it took into account the entire QRS, not just the R-wave. I will be using all the original ECGs to study this hypothesis.
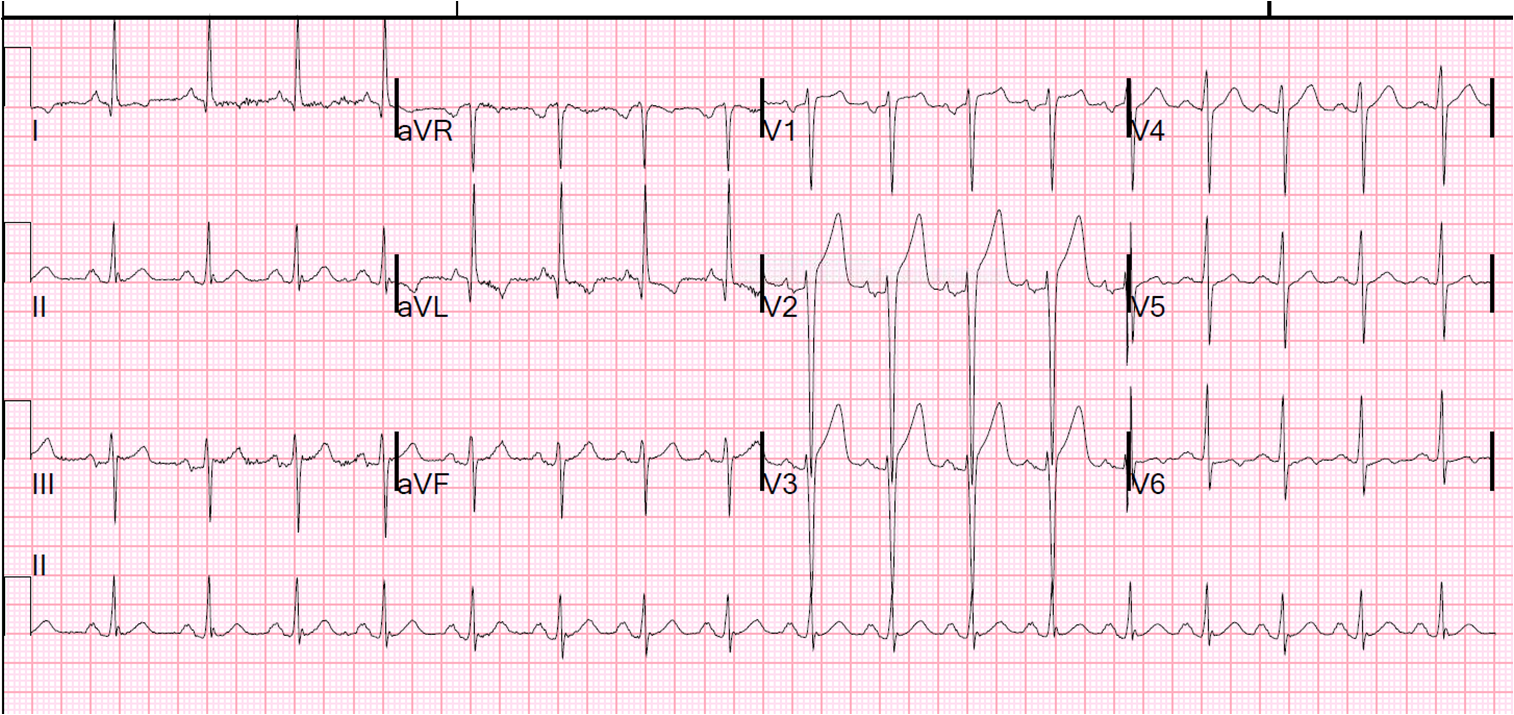
There were no previous ECGs for comparison.
We did a bedside cardiac echo which showed concentric LVH and a well functioning anterior wall. A repeat ECG 30 minutes later was identical. We recommended admission for further evaluation but the patient signed out against medical advice.
Her heart rate came down with IV fluids.
I am quite certain that this is the patient’s baseline ECG.
Lesson:
1. LVH can result in PseudoSTEMI patterns of various morphologies. Here are some others.
2. The formula may give false positives in LVH