This case is presented and written by Vince DiGiulio, (EMT-Critical Care and emergency department tech). As his title shows, he is a tech. Not a paramedic. Not a nurse. Not a doctor. He is a wizard at reading ECGs and is entirely self-taught. He was the ECG tech on this case, and his skills mean that he recognized the pathology on the ECG and could stand there and keep recording them.
A 75 year old female presents with a chief complaint of “reflux.”
Starting about five days ago, a couple of times each day she has experienced a burning sensation behind the lower third of her sternum that is relieved within 10-15 minutes of taking an over-the-counter antacid. She has been diagnosed with GERD in the past and always carries a roll of calcium-carbonate chewables in her purse.
Today she woke with the same pain, but this time it lasted at least an hour before subsiding. A couple of hours later the pain returned, and when it had not diminished after another hour she decided to come to the ED.
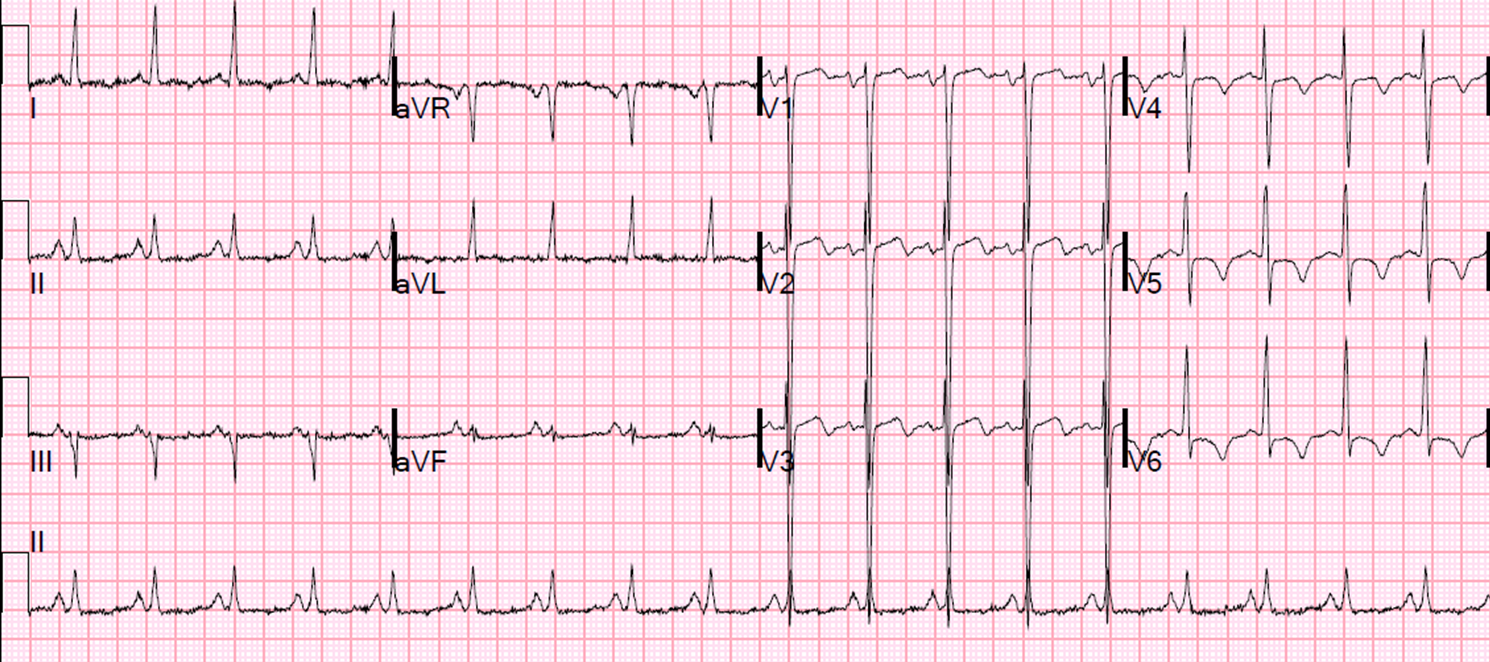
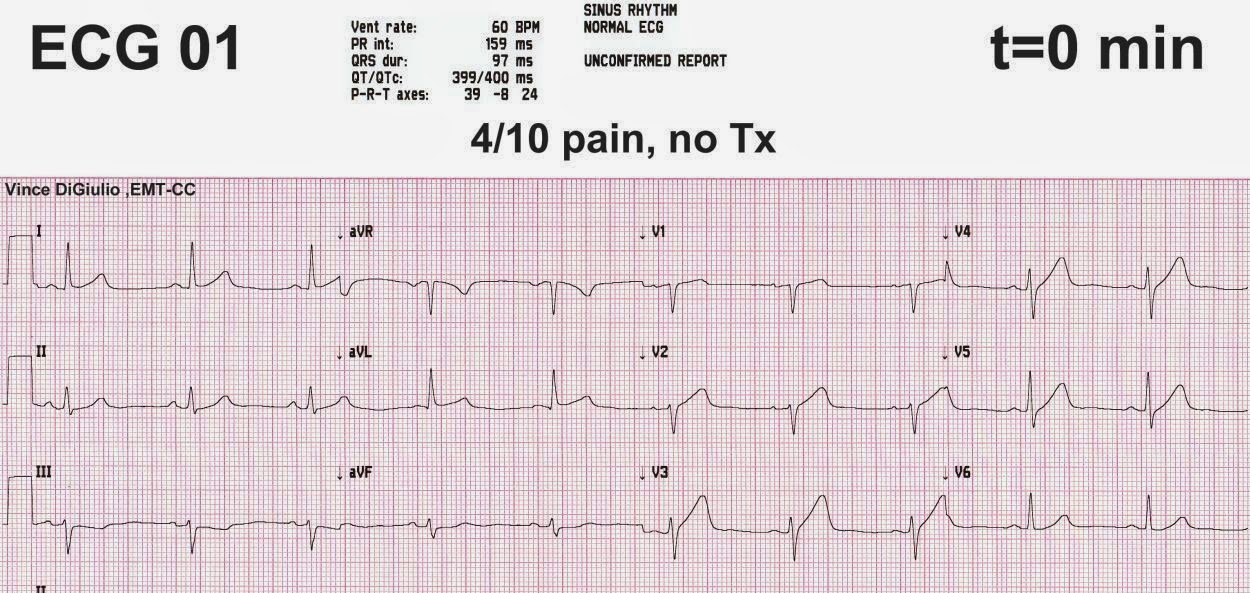
The following ECG is captured on arrival, approximately 90 minutes after onset of the latest episode of pain. The pain has been constant and she rates it as a 4/10.
 |
|
Is |
There is a poor R-wave progression across the precordials (transition is between V4 and V5); subtle ST-elevation in V2-V4, I, and aVL; and reciprocal ST-depression in II, III, and aVF. Additionally, using the BER vs. anterior STEMI calculator on the right side of this page, the equation value of this tracing is 25.4, greater than 23.4 (using measurements of 2.7 mm, 400 ms, and 4.4 mm, respectively). This tracing is diagnostic of anterior subepicardial ischemia, almost always due to LAD occlusion.
As the tech running this EKG, at this point I recognized our patient was almost certainly experiencing a STEMI but knew I would have a tough time convincing our emergency physician, let alone the cardiologist. So, wanting to be sure I was getting the best data possible and not seeing a falsely poor R-wave progression due to incorrect precordial electrode placement, I double checked my stickers (that were all fine) and ran a second ECG exactly 90 seconds later…
 |
|
After only 90 seconds the anterior |
That’s all it took, 90 seconds, with absolutely no change in patient symptoms or condition, and now we have a clearly diagnostic tracing. At this point the cath lab was activated and we finally had time to pull up the patient’s old ECG.
Here is the patient’s basline ECG:
 |
| Normal |
While preparing the patient for transfer, I kept the patient wired and shot the following tracings:
 |
| Only 4 minutes after the first ECG and the ST-elevation keeps growing. Her heart rate has also increased, probably because around this time the doctor was giving the, “I’m concerned about your heart” speech all emergency care providers know so well. |
 |
| We’re now 8 minutes after ECG 01 and the ST-elevation in V3 is almost taller than the R-wave. |
Watch what happens after Nitroglycerin:
 |
| Only minutes after the first SL nitro tablet (0.4 mg) and suddenly the ST/T abnormalities have almost entirely resolved (though the patient is still experiencing the same symptoms). Compared to ECG 01, her anterior T-waves are much more normal in size. The only hints of ischemia are the reciprocal ST- depression in the inferior leads (probably most obvious in aVF) and the upright T-wave in V1, new from her old ECG but very non-specific outside of this scenario. Her equation value is now 23.3, less than 23.4 (using measurements of 1.0 mm, 403 ms, and 5.0 mm). |
Then the T-waves enlarge again!
 |
| This ECG is very similar to ECG 05, but worryingly her anterior T-waves have increased in size again. The patient is still symptomatic, although less so, and there are still the same subtle signs of ischemia present as in ECG 05. Of note, her rate has also slowed significantly secondary to 5mg of metoprolol. Her equation value is now 23.8, greater than 23.4 (using measurements of 1.4 mm, 401 ms, and 4.7 mm). |
Then after another Nitro:
 |
| This tracing is following the second dose of nitro with nearly complete resolution of the patient’s symptoms. Compared to ECG 06, her T-waves have decreased in size again and there seems to be less ST- depression evident in the inferior leads. Even V1 is starting to invert as a return to the patient’s baseline. Outside of the setting of the prior ECG’s, this tracing would be perfectly normal, though there is still some clockwise-rotation of the Z-axis. |
Here Vince has put them all together in an animated GIF to show the progression:

Outcome:
The patient was quickly transferred to the cath lab where a culprit lesion of a large obtuse-marginal artery (surprisingly, it was not LAD, though it would be useful to know more specifics about the coronary anatomy and culprit lesions) was successfully stented with a good outcome. Multi-vessel CAD was also noted, with plans made for CABG sometime after discharge from this hospitalization. After departing the ED, her first troponin-I, drawn eight minutes in at the time of ECG 04, came back at 0.49 ng/mL (ref is less than 0.04 ng/mL)
There are several important take-home points from this case.
First, the ECG 01 was diagnostic of anterior STEMI right from the start. While there might be a couple of true STEMI mimics that can create this picture (stress cardiomyopathy is the best candidate), in the patient presenting with chest pain, this ECG is their ticket to the cath lab.
Second, acute coronary syndrome and myocardial infarction are incredibly dynamic processes, with vessels occluding, de-occluding, and spasming on a sometimes rapid basis. In this case it took only 90 seconds, with no change in patient symptoms, for her ECG abnormalities to progress from very subtle to markedly abnormal. Don’t be afraid of serial ECG’s, even if the patient’s symptoms are constant.
Related to that, and this is especially directed towards prehospital providers, don’t ever give nitro without first running a 12-lead. It only took one SL nitro for this patient’s ECG to go from an obvious anterior STEMI in ECG 04 to completely non-diagnostic in ECG 05. If you only had the latter ECG to go on, you would never know that this patient was actually experiencing a true anterior MI. It might not happen too often (see this case: https://drsmithsecgblog.com/2011/07/wait-until-after-ecg-to-
give.html), but it’s vitally important information.
Finally, one of the nurses working on this case was shocked when I showed her the rapid changes in the patient’s ST-elevation after the patient had been transferred. She had been closely following the rhythm strip on the three-electrode, three-lead cardiac monitor, and had noticed absolutely no changes or even abnormalities aside from a small amount of ST-depression. This is because she was monitoring lead II, which, if you look back, was equally unimpressive across every ECG I shot. You cannot monitor just a single lead in ACS patients, especially when anterior MI is a concern. These patients need, at the very least, five-electrode cables capable of monitoring the augmented leads along with a chosen precordial lead, if not continuous 12-lead monitoring. As this case demonstrates, the ECG’s of ACS patients can change too rapidly, independent of patient symptoms, to warrant anything less.