This 58 year old man presented at noon with chest pain that began the previous evening and became constant less than one hour prior.
 |
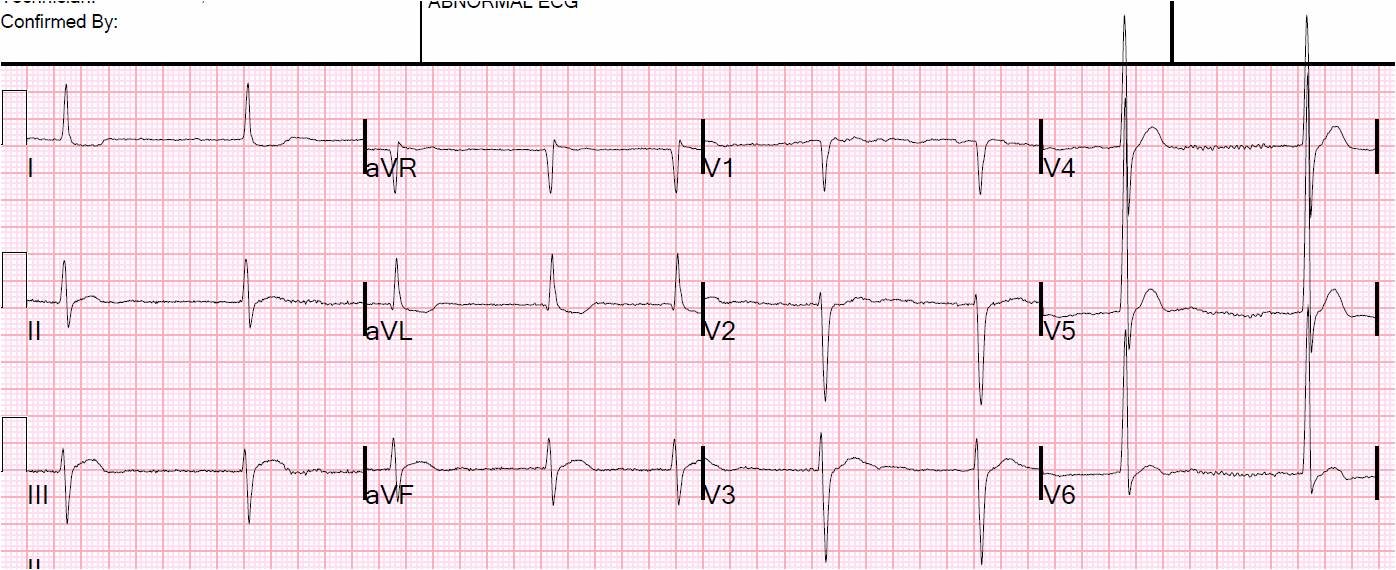
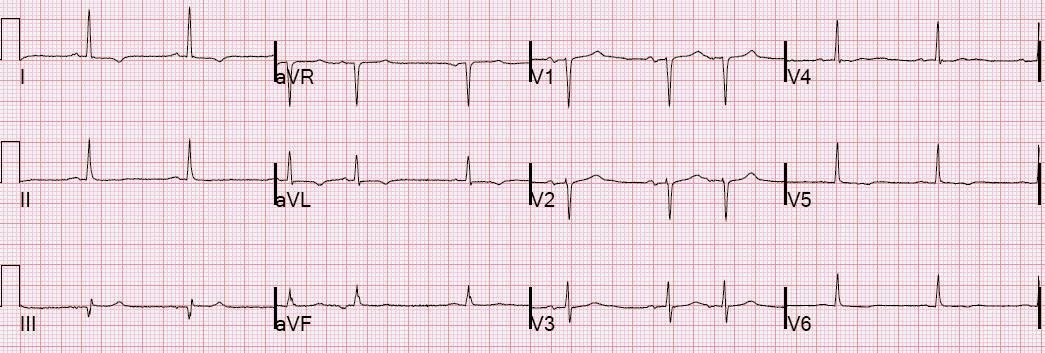
| Now there is still sinus rhythm but with 2 complexes that are PACs with aberrancy [not PVCs (thanks to VinceD for correcting me on that!)]. There is subtle ST depression in “inferior” leads II and aVF. This should always alert to ST elevation in the opposite, high lateral, leads especially aVL. Looking at aVL, there is indeed subtle ST elevation and also in lead I. |
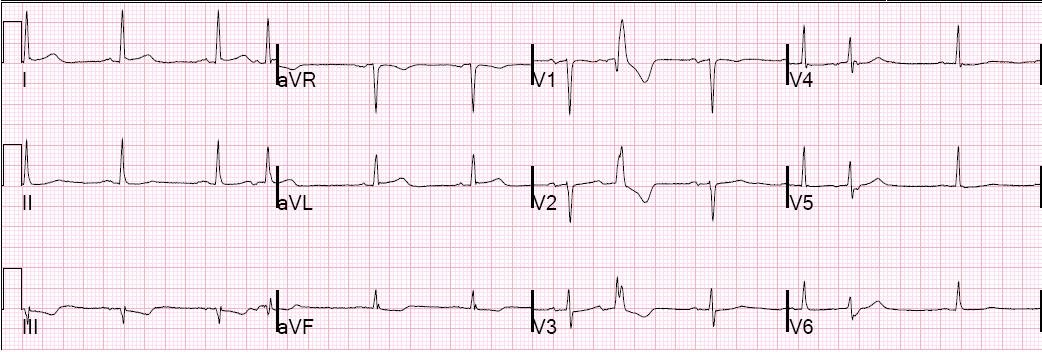
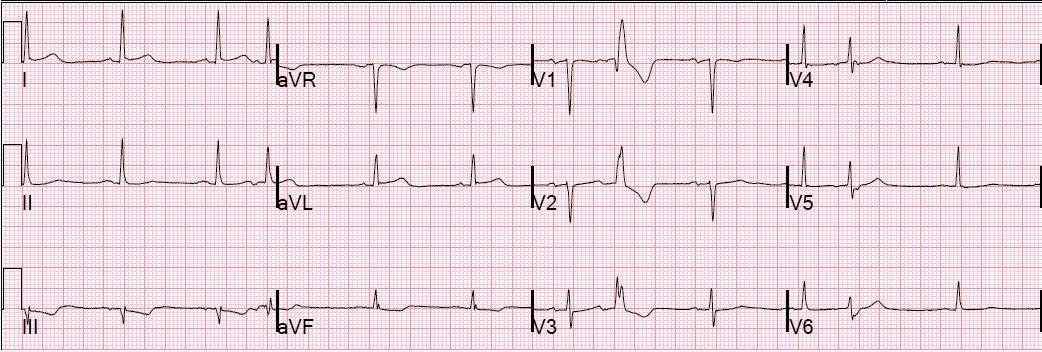
Here is the previous ECG for comparison:
 |
|
|
Subendocardial ischemia may have ST segment depression, but it does not reliably localized to any wall. “Inferior” ST depression is really reciprocal to high lateral ST elevation.
The chest pain resolved with nitroglycerine, the cath lab was activated, and a 99% LAD D2 (large second diagonal off the LAD) was found and stented.
Subsequently, there was no wall motion abnormality and the maximum troponin I was 1.0 ng/ml.
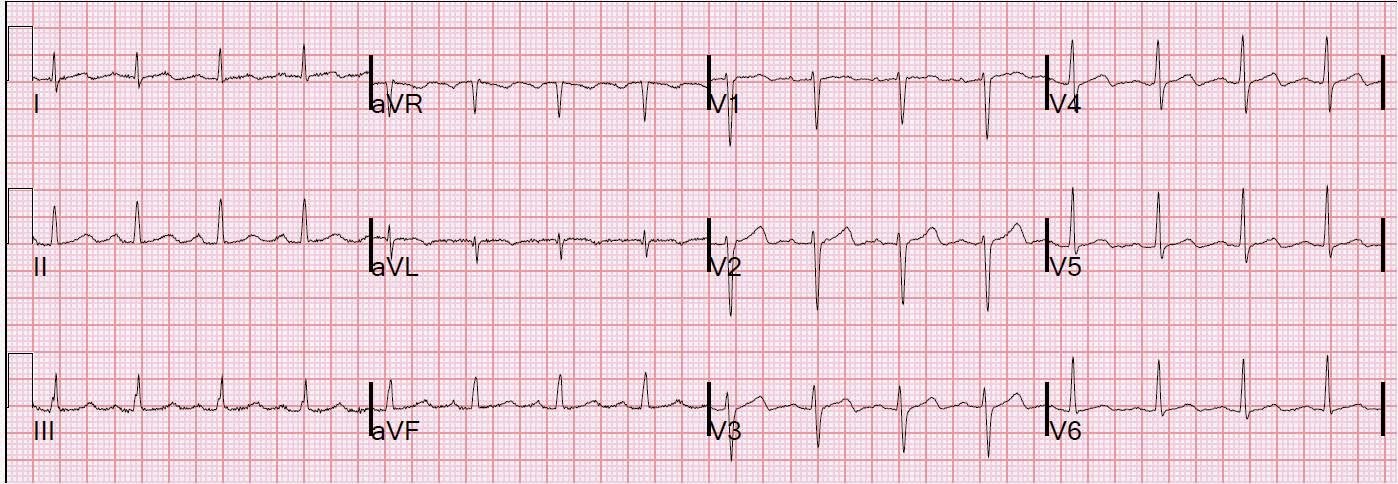
Here is a followup ECG 42 hours later:
 |
|
|
1) ST depression in III and aVF should be assumed to be reciprocal to high lateral ST elevation
2) This ST depression may be the most visually arresting part of the ECG
Here you can find other similar cases:
https://drsmithsecgblog.com/2010/08/35-yo-woman-with-lad-occlusion.html