A middle-aged patient called 911 for 1 hour of chest pain.
He was hemodynamically stable.
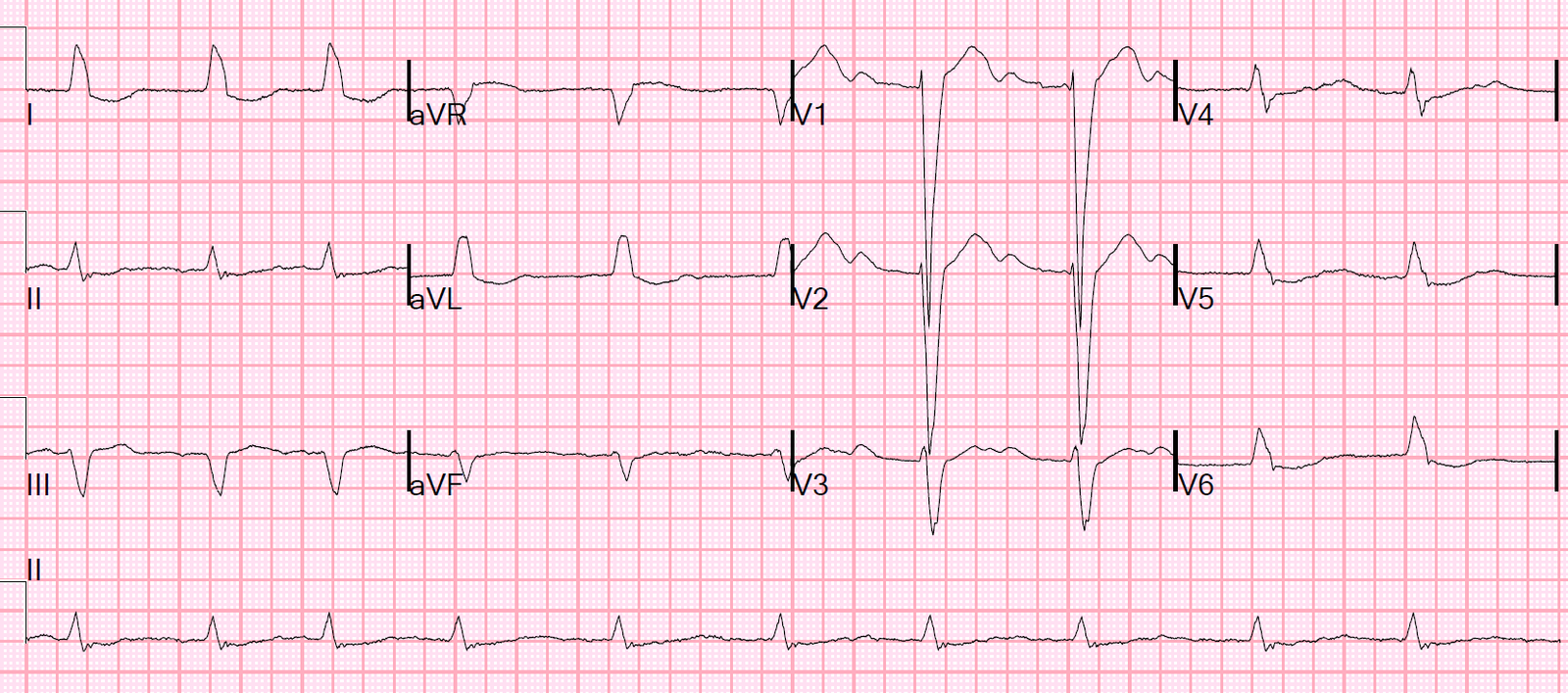
Here is the prehospital ECG:
 |
| Obvious inferior MI, but also with STE in V3-V6 |
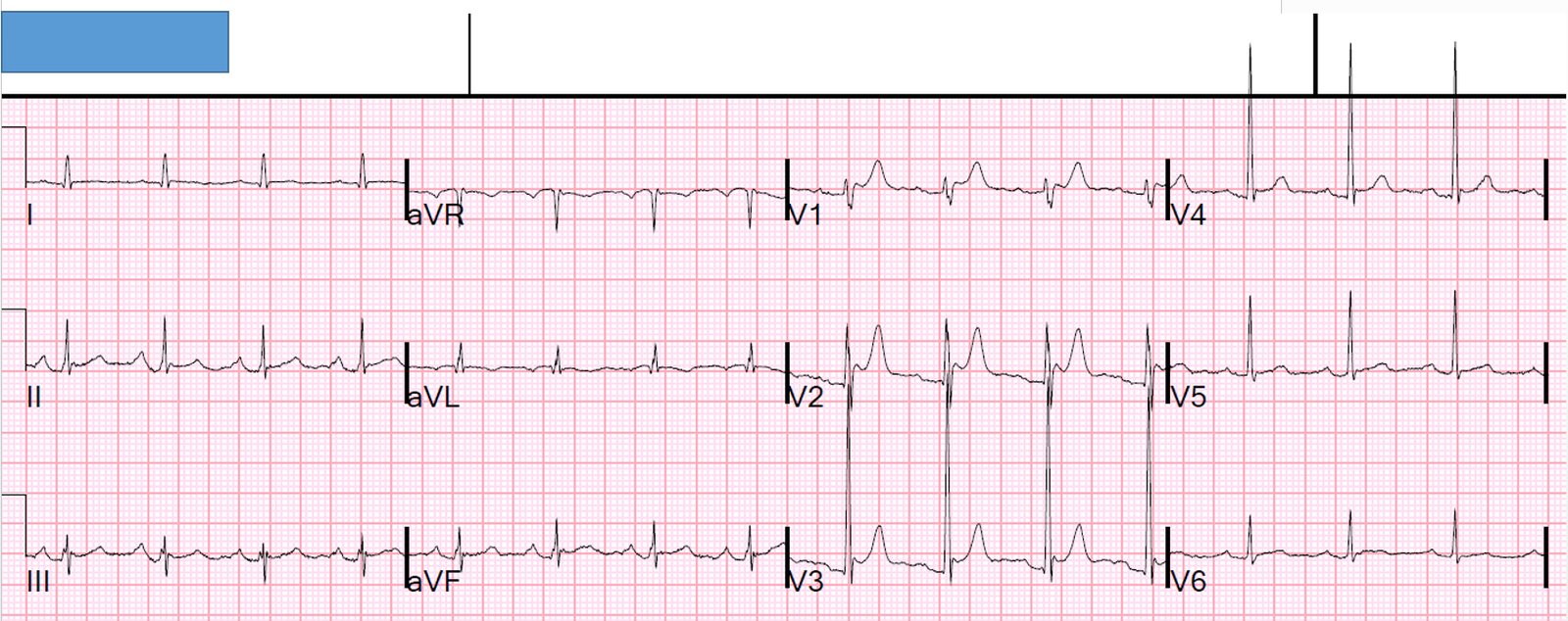
Here is the first ED ECG:
 |
| Again, inferior and lateral STEMI. Is there any right ventricular (RV) MI? |
85% of inferior MI are due to RCA occlusion. Even the majority of inferolateral MI are due to RCA occlusion. The RCA may have a large lateral branch.
RV MI is caused by RCA occlusion proximal to the RV marginal branch, especially when there are no collaterals from the LAD to the RV.
We showed that, if there is zero ST depression in lead V2, that lead V1 is 85% sensitive for RVMI. When there is STD in V2, only 35% have any STE in V1.
We should have titled it: In Inferior Myocardial Infarction, for diagnosis of RV MI, ST elevation in lead V1 is only sensitive in the absence of ST depression in V2; lead I is not reliable.
We care about RV MI because it can cause RV failure, with shock and hypotension.
But only a minority of patients with RV MI have these adverse hemodynamics, and an even smaller number with proximal RCA occlusion have these hemodynamics because they may have blood supply from LAD collaterals.
Is it important to diagnose RV MI here?
Probably not so much. He is hemodynamically stable.
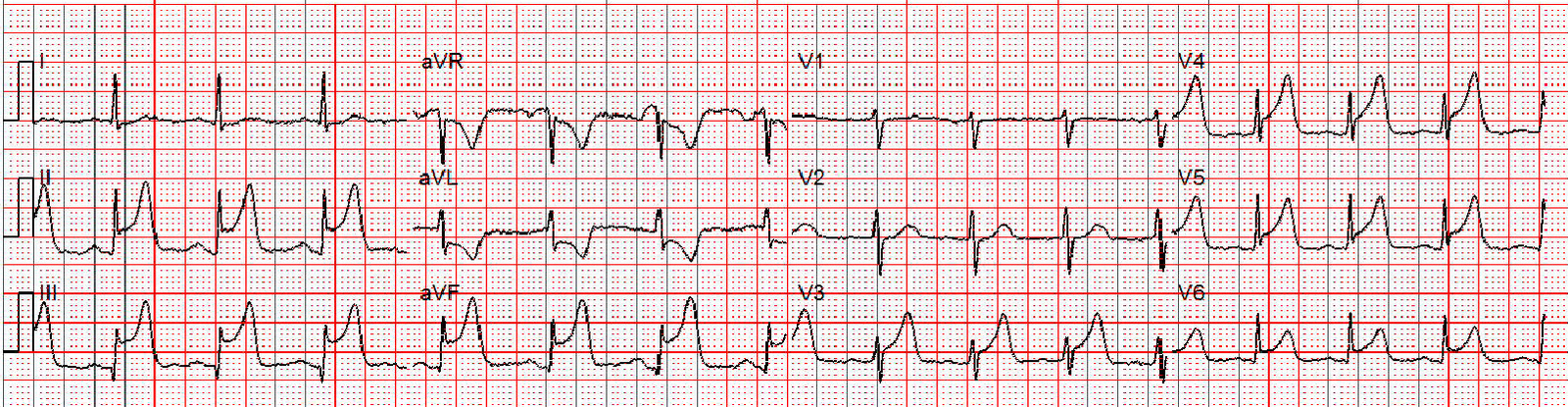
Nevertheless, we took a look with a right sided ECG. Here it is:
 |
| V1-V6 are really V1R (=V2) to V6R There is STE in V3R to V6R. This is diagnostic of RV MI. This is one of the 15% of RVMI that have zero STD in V2 but no STE in V1. Perhaps the absence of STE in V1 (=V2R) is a good prognostic sign? Perhaps it means that the critical anterior wall of the RV is not ischemic, even if more right lateral portions are ischemic? This is pure speculation. |
The patient went to the cath lab and had a proximal RCA occlusion opened and stented. He was never hypotensive.
Here is the post PCI ECG:

Angiogram
Acute Inferior ST elevation MI.
Culprit is 100% occlusion of the Proximal RCA .
LMCA: The LMCA has mild plaque.
LAD: No angiographic significant obstructive disease.
LCx: No angiographic significant obstructive disease.
RCA: RCA has Normal take off. The Proximal segment of the RCA has 100% disease.
Lesion on Prox RCA:
Echo:
The estimated left ventricular ejection fraction is 41 %.
Left ventricular hypertrophy concentric .
Regional wall motion abnormality-distal septum and apex.
Regional wall motion abnormality-distal inferior wall.
Regional wall motion abnormality-anterolateral.
ADDITIONAL REMARKS
Findings c/w ischemia/MI in vascular territory of LAD, proximal to a diagonal branch.
(However, concomitant MI/ischemia in distal PDA/watershed territory cannot be excluded)
Learning points:
1. Inferior STEMI is usually caused by RCA occlusion
2. RCA occlusion may be proximal to the RV marginal branch
3. Proximal occlusions may or may not result in ECG or hemodynamic evidence of RV MI
4. When there is no ST depression in lead V2 AND a proximal RCA occlusion, there is STE in V1 approximately 85% of the time.
5. STD in Lead I is not useful to diagnose RV MI except to differentiate RCA from circumflex occlusion. (RVMI can only occur with RCA occlusion)
6. Diagnosis of RV MI is important in the presence of hemodynamic instability