This 50-something otherwise healthy male presented with one hour of epigastric and lower chest pain.
Here is his initial ECG:
 |
| What do you think? The QRS is 90 ms and the QTc is 400 ms. |
There is ST Elevation (STE) in II, III, aVF, with reciprocal ST depression in aVL. There is also ST depression in V2 and V3. V2 and V3 almost always have some amount of normal ST elevation, and since posterior MI is associated with inferior MI, you must make notice of this and think it is probably an inferior posterior MI.
However, II, III, and aVF have what appear to be J-waves at the end of the QRS. If these are J-waves, then couldn’t the inferior ST elevation be due to early repol?
1. When there is ST depression in aVL, early repol as a cause of inferior STE is VERY unlikely
2. These do NOT appear to be J-waves.
Instead, these are spikes at the end of the QRS in II, III, and aVF. There is also an unusual wave at the end of the QRS in I and V6 .
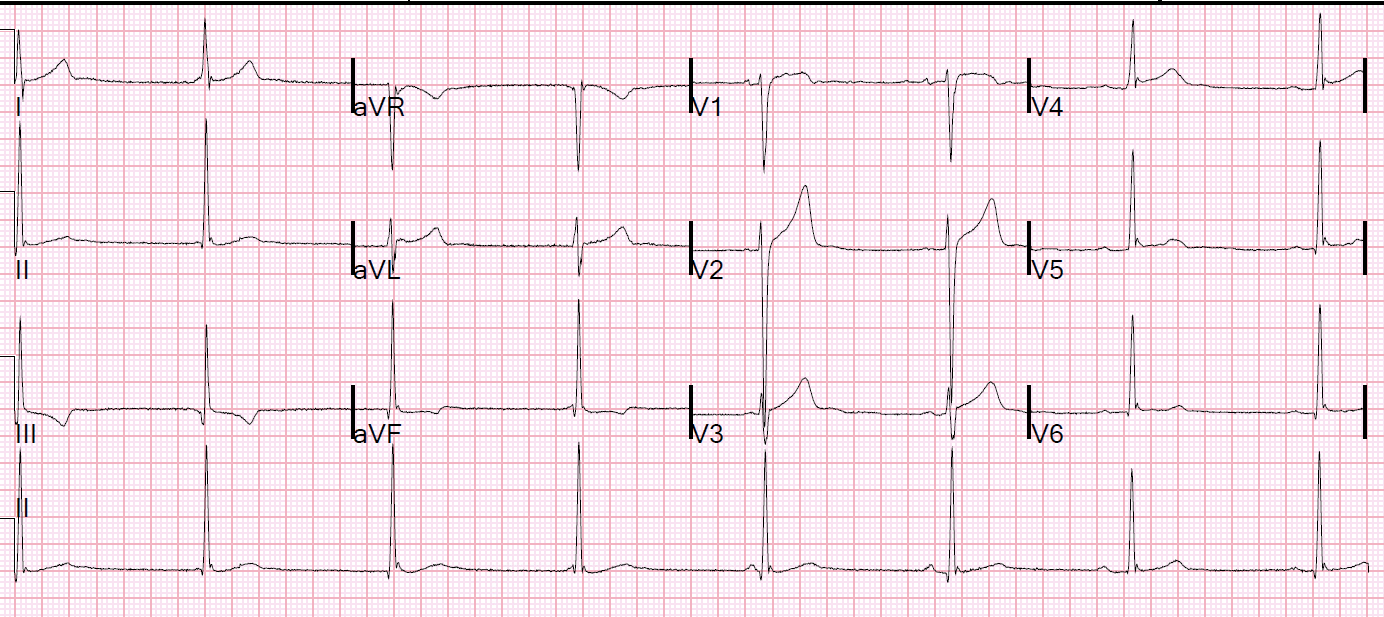
These are what J-waves look like:
 |
| This is inferior and lateral early repolarization. The waves in II, V5, and V6 are typical J-waves. There is typical slurring of the J-point (end of QRS, beginning of ST segment) in lead III Note absence of ST depression anywhere. Note that there is some ST elevation in V2 and V3, which is normal (ST depression in these leads is very abnormal) |
So the above first ECG is nearly diagnostic of inferior and posterior MI.
One of our fine interns, Daniel Lee, who is also an ECG whiz, found this paper from 2013 and brought it to my attention:
The delayed activation wave in non-ST-elevation myocardial infarction.
He also wrote about it in this post:
OMI Can be Diagnosed by “Pseudonormalization of ST Segments”
In this paper, they describe a new “N-wave” in NonSTEMI that helps in determining the infarct artery. When present, the infarct artery is more likely to be the circumflex. They do not study whether this wave differentiates between MI and non-MI, between STEMI and NonSTEMI, or between OMI and NOMI.
The N-wave was defined as:
(1) a notch or deflection in the terminal QRS complex of the surface ECG
(2) the height of notch or deflection is at least 2 mm (the point of deflection was measured with reference to the PR segment);
(3) a continuous change of the notch (the point of deflection shifted at least 2 mm with
reference to the PR segment in at least 2 leads within 24 hours, even disappeared or merged with the S-wave)
(4) with a prolongation of QRS duration in these leads.
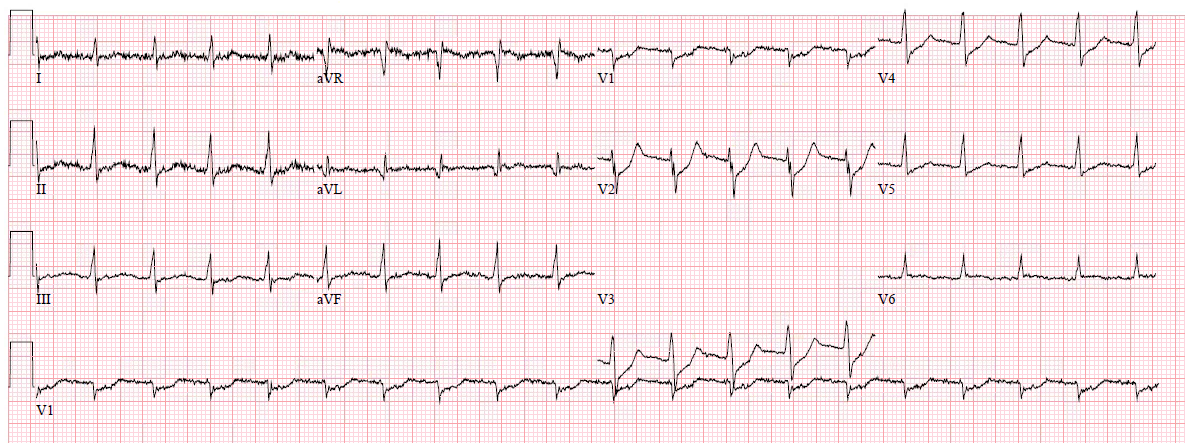
Here is an ECG with N-waves, from the article:

Are these N-waves in our ECG? They do not appear to be wide enough, but they still might be.
Case continued:
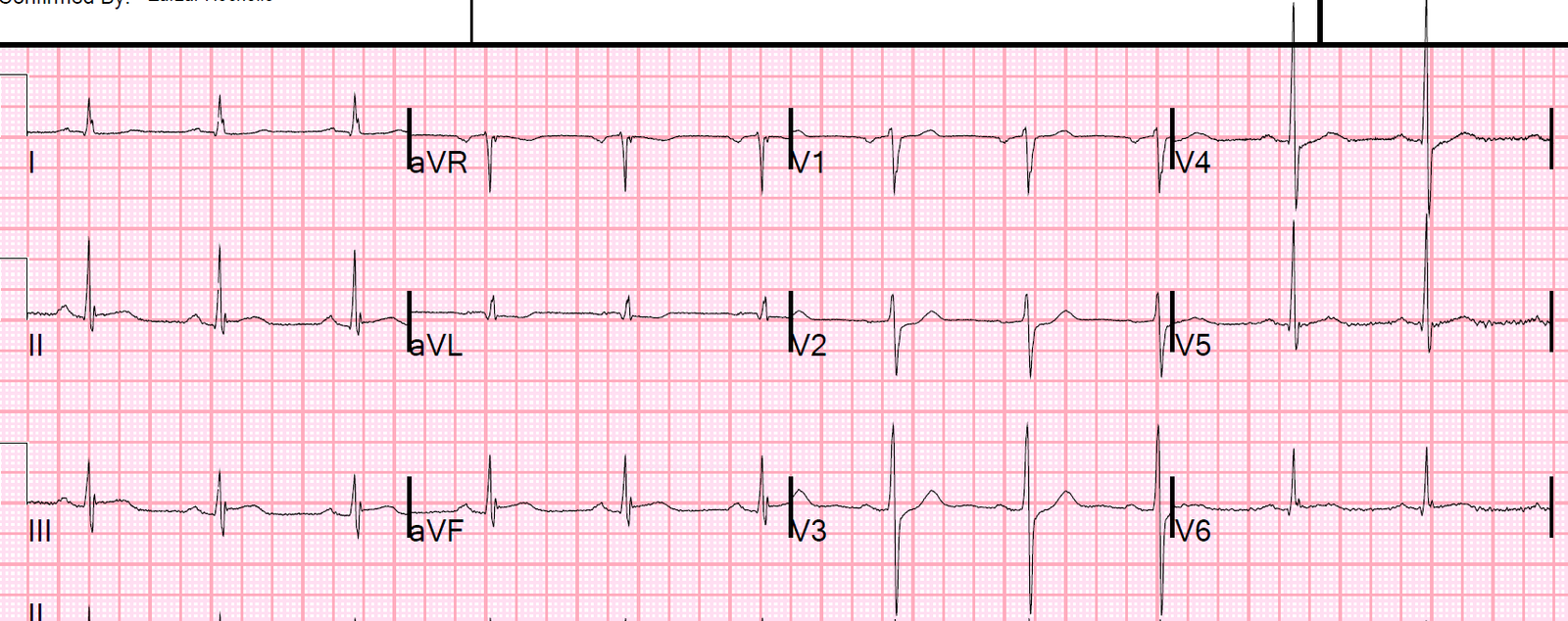
The first troponin I returned at 0.087 ng/mL (elevated). Another ECG was recorded:
 |
| Hardly any changed, though the computer now measures the QRS at 116 ms. |
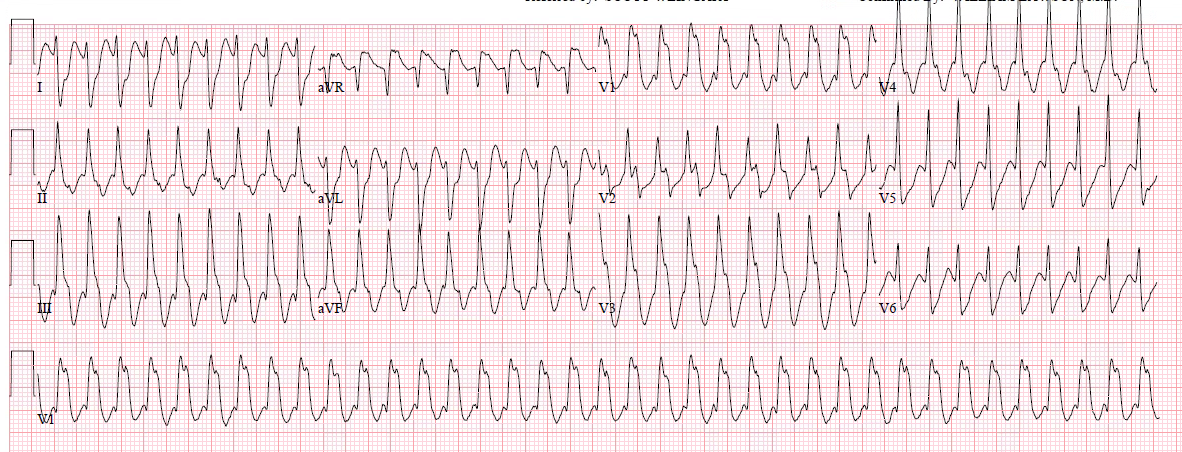
Approximately 45 minutes after this, the patient’s pain became much worse. Another ECG was recorded:
 |
| Obvious inferior, posterior, lateral STEMI What is the infarct artery? This is hard to tell. Of all inferior STEMI, 85% are due to RCA. When there is ST depression in lead I, that percentage is higher. When there is no STE in I, the percentage is lower, maybe 65% (such that the % of circumflex is higher at about 35% rather than 15%) If these spikes are indeed delayed activation waves, then this feature would further favor the circumflex artery. |
The cath lab was activated.
A 100% occlusion on of the circumflex, proximal to the first obtuse marginal, was found, opened, and stented.
This case produces more questions than answers
1. Are “Delayed Activation Waves” a real phenomenon?
2. If so, were the waves in this case actually “Delayed Activation Waves” (N-waves)??
3. Can delayed activation waves be used to differentiate non-ischemic ST elevation from ischemic ST elevation?
4. Can they be used to differentiate OMI from NOMI?